Chiropractic Care and Digestive Wellness

How the Spine, Nerves, and Stress Can Affect Your Gut
Digestive problems are common. People often experience symptoms such as bloating, constipation, diarrhea, heartburn, reflux, or “mixed” symptoms that fluctuate in frequency. Sometimes the trigger is obvious (food choices, alcohol, certain medications, poor sleep). Other times, the pattern feels confusing: symptoms flare during stressful weeks, after long hours sitting, or when back and rib pain is also acting up.
Many chiropractors and integrative clinics talk about a “gut–brain–spine” connection. The basic idea is simple:
- Your brain and spinal cord help control digestion through the autonomic nervous system (your “automatic” control system).
- The thoracic (mid-back) and lumbar (low-back) spinal levels are closely linked to nerve pathways that influence gut motility, secretion, and blood flow.
- Pain, muscle guarding, poor breathing mechanics, and chronic stress can push the body into a more “fight-or-flight” pattern, which often slows digestion and increases sensitivity.
Some people report digestive improvements during chiropractic care. Research is mixed: there are case reports and some clinical studies suggesting benefit for certain problems, but reviews conclude that the evidence is not strong enough to claim that chiropractic “treats” GI disease. The most accurate, helpful approach is to understand what chiropractic may support, what it cannot replace, and how an integrative plan can be built around safe, evidence-informed steps.
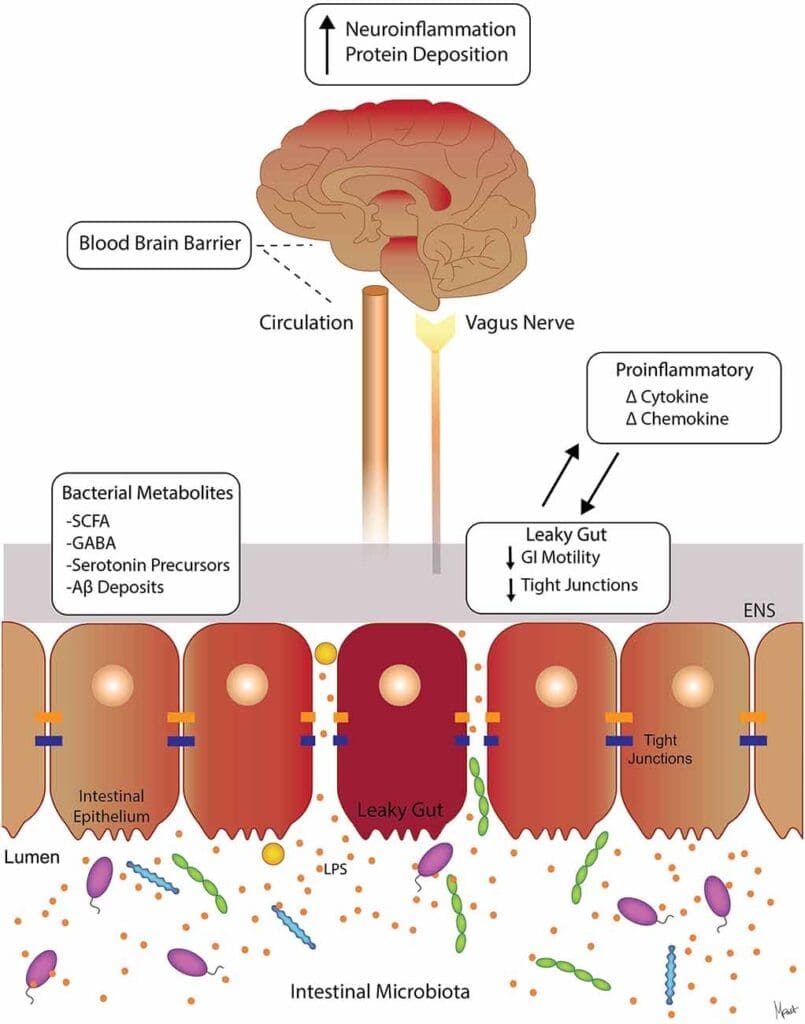
The Gut–Brain–Nerve Connection in Plain Language
Digestion is not just “your stomach doing its job.” It’s a coordinated rhythm involving:
- Muscle contractions (motility/peristalsis)
- Sphincters opening and closing at the right time
- Stomach acid and digestive enzymes
- Blood flow to digestive organs
- Immune signals and inflammation control
- Nerve signals between the gut, spinal cord, and brain
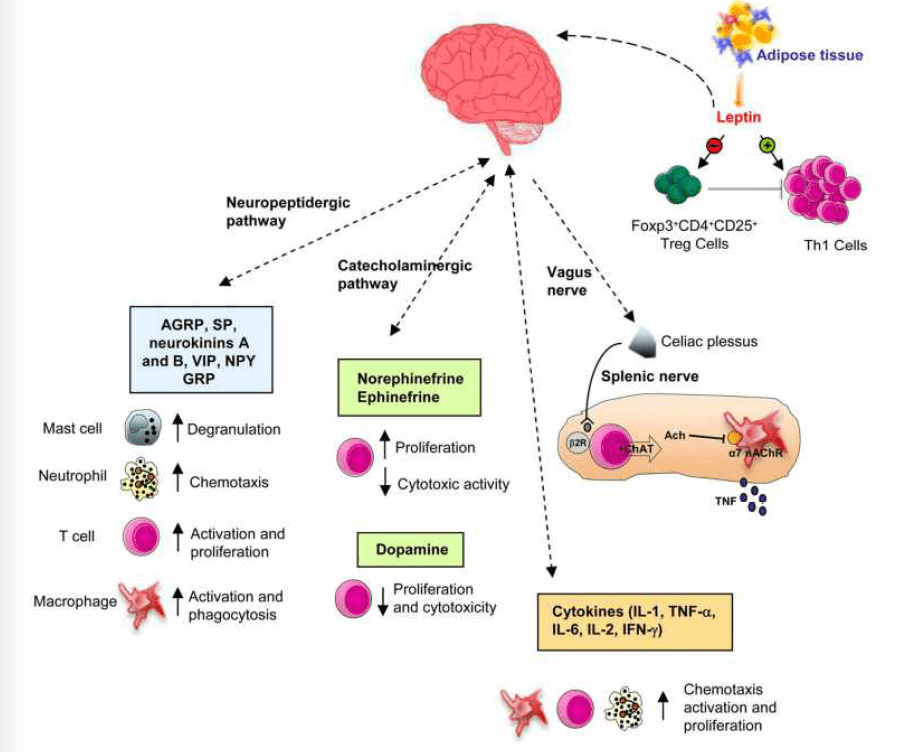
Two major nerve control systems matter here:
- Enteric nervous system (ENS): the “local” nerve network in the gut
- Autonomic nervous system (ANS): the “command” system that shifts digestion up or down depending on stress and safety cues
When stress stays high, the body tends to lean toward sympathetic dominance (“fight-or-flight”), which can reduce normal digestive activity. When the body feels safer and calmer, it can shift toward parasympathetic activity (“rest-and-digest”), which is strongly linked to the vagus nerve.
Why the thoracic and lumbar spine are mentioned so often
From a physiology standpoint, it’s true that sympathetic control of the GI tract involves spinal cord levels in the thoracic and lumbar regions. For example, research reviews describe sympathetic pathways to the gut arising from thoracic and lumbar spinal cord segments, with different regions influencing different parts of the GI tract.
That does not automatically prove that every spinal joint problem causes gut disease. But it does help explain why posture, rib mobility, diaphragm function, and stress-related tension patterns can be linked with digestive comfort and regularity.
What Chiropractors Mean by “Subluxation” and Why People Connect It to Digestion
In chiropractic, “subluxation” is often used to describe joint dysfunction (restricted motion, irritation, altered mechanics) that may influence muscle tone and nervous system balance.
In mainstream medicine, the word “subluxation” usually means a partial dislocation seen on imaging, which is different. Because the term is used differently across fields, it’s better to focus on the practical, testable issue:
- Is there restricted spinal or rib motion?
- Is there muscle guarding?
- Is posture or breathing mechanics limited?
- Is pain and stress high enough to affect sleep, movement, and digestion?
Many chiropractic articles argue that spinal adjustments may help digestion by reducing “nerve interference” and supporting the body’s normal control systems.
How Chiropractic Care May Support Digestive Wellness
Better movement and less guarding can support gut motility
The intestines move food by coordinated muscle contractions. If someone is stuck in a pattern of:
- shallow breathing
- tight abdominal wall
- stiff mid-back and ribs
- high stress and poor sleep
…then gut motility can feel “off.” Some clinics report that adjustments, along with soft-tissue work and breathing retraining, may help people feel less tight and more regular.
Common supportive steps used alongside adjustments include:
- rib and thoracic mobility work
- diaphragm breathing practice
- gentle walking after meals
- hydration and fiber adjustments (when appropriate)
- stress regulation habits (sleep, pacing, recovery)
(These lifestyle steps matter because digestion is highly responsive to stress load and daily rhythm.)
Stress regulation is a big “hidden” gut factor
A major integrative message across many sources is that chiropractic care may support digestion, in part, by helping the body shift out of constant fight-or-flight patterns.
This does not mean an adjustment magically “fixes” IBS. It means care that reduces pain, improves sleep, and supports calmer breathing can indirectly help the gut function more normally.
Posture and spinal mechanics can affect breathing and pressure systems
Breathing and digestion share anatomy and pressure control:
- The diaphragm influences abdominal pressure.
- Slumped posture can reduce rib expansion and change abdominal pressure patterns.
- Pressure changes can influence reflux symptoms in some people.
Dr. Alexander Jimenez often discusses how posture, thoracic mechanics, breathing patterns, and stress physiology can affect digestive comfort in an integrative model.
Conditions People Commonly Ask About
Irritable Bowel Syndrome (IBS)
IBS is complex. It involves gut sensitivity, changes in motility, brain–gut signaling, stress response patterns, and sometimes food triggers.
Some chiropractic and wellness sources suggest that supporting nervous system regulation may help reduce the severity of IBS symptoms for some individuals.
There are also clinical studies on spinal manipulation approaches in IBS populations. For example, PubMed-indexed trials exist that report symptom improvements after spinal manipulation protocols in IBS groups—though results, methods, and generalizability can vary, and this does not mean chiropractic is a stand-alone cure for IBS.
If you have IBS, an integrative plan often works best:
- rule out red flags (bleeding, anemia, unexplained weight loss, fever)
- identify triggers (sleep loss, stress spikes, certain foods)
- build a steady routine (meals, hydration, movement)
- consider guided nutrition strategies with a qualified clinician
- use supportive manual therapy for mobility, pain, and stress load (when appropriate)
Constipation
Constipation can be driven by diet, hydration, fiber tolerance, pelvic floor issues, thyroid problems, medications, or low activity. Some case reports in the literature describe improvements in bowel movement frequency alongside chiropractic care, but case reports are not the same as large, high-quality trials.
If constipation is chronic, an integrative clinic may also look at:
- pelvic and hip mechanics
- breathing and abdominal pressure strategy
- activity level (walking is underrated)
- medication review
- lab work or referral when appropriate
Acid reflux/GERD-like symptoms
Some chiropractic sources claim spinal adjustments may help reflux by influencing posture, rib mechanics, stress response, and possibly vagal/autonomic balance.
However, when it comes to GERD specifically, the published chiropractic literature is often described as sparse, with limited case reports rather than definitive trials.
Important: If you have frequent reflux, chest pain, trouble swallowing, black stools, vomiting blood, or unexplained weight loss, it needs medical evaluation.
What the Research Says (Supportive Signals + Real Limits)
It’s easy to find confident marketing claims online. The science picture is more mixed.
Supportive signals
- A 2015 review in Explore (NY) examined chiropractic care for GI conditions and summarized a range of study types (from case reports to trials), with many reports describing mild to moderate symptom improvement and few adverse effects reported in those papers.
- Some IBS trials report improvements in symptom scores with spinal manipulation protocols.
Cautionary conclusions
- A 2011 review by Edzard Ernst concluded there was no supportive evidence that chiropractic treatments are effective for gastrointestinal problems (based on the evidence base as reviewed at that time).
The most honest takeaway
Chiropractic care may be a supportive strategy for certain people—especially when digestive symptoms are strongly tied to stress, pain, posture, breathing mechanics, and overall nervous system load. But it should be positioned as part of a broader plan, not as a guaranteed “treatment” for GI disease.
An Integrative Chiropractic Approach to Digestive Wellness
Many clinics combine adjustments with practical lifestyle steps. Across your provided resources, common themes include spinal alignment, nervous system support, stress reduction, and nutrition pairing.
A practical, patient-friendly plan (often used in integrative settings)
Step 1: Screen for red flags
- blood in stool, black stools
- persistent fever
- severe or worsening pain
- unexplained weight loss
- vomiting that won’t stop
- trouble swallowing
- anemia or significant fatigue
Step 2: Look for mechanical drivers
- rib and thoracic stiffness
- low-back and pelvic motion limits
- abdominal wall guarding
- shallow breathing and poor diaphragm function
- forward-head posture with upper back rounding
Step 3: Start with conservative care
- chiropractic adjustments (as appropriate)
- mobility work for the thoracic spine and hips
- soft-tissue techniques to reduce guarding
- breathing drills to support “rest-and-digest.”
Step 4: Pair with gut basics
- consistent meal timing
- hydration
- fiber changes based on tolerance (some IBS patients do worse with sudden fiber increases)
- protein + plants + healthy fats
- reduce ultra-processed triggers when possible
Step 5: Track outcomes
- stool frequency/consistency
- reflux days per week
- bloating severity
- sleep quality
- stress rating
- pain and mobility changes
Helpful tracking tip: Don’t track 20 things. Track 3–5 simple measures for 2–4 weeks.
Dr. Alexander Jimenez’s Clinical Lens (Chiropractic + Nurse Practitioner + Functional Medicine)
Dr. Alexander Jimenez, DC, APRN, FNP-BC, frequently frames digestive wellness as part of a bigger integrative picture—especially the overlap between:
- spinal mechanics and posture
- stress physiology and nervous system balance
- nutrition strategies that reduce inflammation load
- step-by-step habits patients can maintain
On his clinical site, gut and intestinal health are described in terms of digestion, absorption, assimilation, and whole-body impact, emphasizing how gut function connects to broader wellness.
In his integrative “gut health and detox” discussions, he also highlights practical components such as calming the system, supporting daily digestion, and combining chiropractic care with nutrition and lifestyle support.
That dual-scope model (chiropractic + NP lens) is especially useful when digestive symptoms overlap with:
- chronic pain and inflammation patterns
- stress-related sleep disruption
- medication considerations
- the need to rule out medical red flags while also building conservative, day-to-day solutions
Safety Notes: When Chiropractic Is Not the Right Tool (or Not Enough)
Chiropractic care is generally considered safe when performed by a licensed professional for appropriate conditions, but no treatment is risk-free. Mild soreness can happen, and rare serious events have been discussed in safety reviews.
Seek medical care quickly if you have:
- severe abdominal pain with fever
- persistent vomiting
- blood in stool or black/tarry stool
- chest pain, fainting, or shortness of breath
- trouble swallowing or choking
- unexplained weight loss
And if you have a known GI diagnosis (Crohn’s, ulcerative colitis, celiac disease, significant GERD complications), chiropractic care should be considered adjunctive—not a replacement for medical management.
Bottom Line
Chiropractic care may support digestive wellness in a few realistic ways:
- improving thoracic/lumbar mobility and reducing muscle guarding
- supporting calmer breathing mechanics and stress regulation
- reducing pain-driven stress load that can disrupt gut function
- fitting into a broader integrative plan that includes nutrition, sleep, movement, and medical screening when needed
The evidence base is mixed. Some studies and case reports suggest symptom improvement in certain GI complaints, while other reviews argue evidence is insufficient for firm claims. The best approach is honest, practical, and patient-centered: use chiropractic care as one supportive tool inside a full, common-sense digestive wellness strategy.
References
- Abundant Life Chiropractic. (2024, October 7). Chiropractic adjustments and gut health: Key connections explained
- Angus, K. (2015). What effect does chiropractic treatment have on gastrointestinal (GI) disorders: A narrative review of the literature
- Atlas Injury to Health. (2025, April 25). The benefits of chiropractic care for digestive health: Reducing inflammation and improving gut function
- Breit, S., Kupferberg, A., Rogler, G., & Hasler, G. (2018). Vagus nerve as modulator of the brain–gut axis in psychiatric and inflammatory disorders
- Browning, K. N., & Travagli, R. A. (2014). Central nervous system control of gastrointestinal motility and secretion and modulation of gastrointestinal functions
- Chiro Health & Wellness. (n.d.). Can chiropractic care help with digestive issues?
- Chiro Health & Wellness. (n.d.). Can chiropractic care improve digestive issues like GERD?
- De Integrative Healthcare. (2020, October 10). Chiropractic care and gut health: Getting to the bottom of distressing digestive issues
- Ernst, E. (2011). Chiropractic treatment for gastrointestinal problems
- Grove Chiropractic. (2025, April 24). Integrating chiropractic care with nutrition for optimal wellness
- HNH Chiropractic. (n.d.). The gut-brain connection: How chiropractic care can help improve digestive health
- Jimenez, A. (n.d.). Gastrointestinal stress and digestion
- Jimenez, A. (n.d.). Gut and intestinal health (category archive)
- Jimenez, A. (n.d.). Chiropractic gut health and detox for bloating & reflux relief
- Living Well Bainbridge. (n.d.). How chiropractic adjustments can improve digestion
- Qu, L., Xing, L., Zhang, H., & others. (2012). Irritable bowel syndrome treated by traditional Chinese spinal orthopedic manipulation: A randomized controlled trial
- UHealth Chiropractic. (2024, November 13). Can a chiropractor help with digestive problems?