Back pain is a big issue for many people. In the United States, up to 80% of adults deal with low back pain at some point in their lives. This is one of the leading reasons for missed work and doctor visits. People often seek ways to manage pain, identify treatments, and modify daily habits to maintain health. In El Paso, Texas, where many folks are active, work in factories, or drive a lot, questions about back pain are common, too. Issues like sciatica, herniated discs, and spinal stenosis show up often due to local lifestyles. This article examines key questions about back health, such as wearing backpacks safely, treatment options, and tips for relief. It draws on authoritative sources to provide clear answers.
Is It Okay to Wear a Backpack?
Yes, wearing a backpack is fine if done right. Backpacks can help carry items without much strain, but improper use can harm your back. Heavy or poorly fitted packs can cause muscle fatigue, bad posture, and even chronic pain. They do not cause scoliosis, a spinal curvature that affects approximately 4% of people, typically beginning in adolescence (Scoliosis SOS, n.d.). Instead, overloads lead to slouching, shoulder pain, and lower back issues.
To spread weight and avoid strain:
Keep the pack light: Aim for no more than 10-15% of your body weight. For a 150-pound person, that’s up to 22.5 pounds.
Use both straps: Adjust them so the pack sits in the middle of your back, not sagging low. This keeps the weight even.
Pack smart: Put heavy items at the bottom and close to your back. Clean out extras often.
Add support: Look for packs with padded straps, a back panel, and a waist strap to share the load with your hips.
Lift correctly: Bend your knees, not your back, when lifting it.
These steps reduce risks like nerve irritation or misalignment (Ireland Clinic, n.d.). In El Paso, where people carry work tools or drive with bags, even weight helps prevent daily aches.
Spinal Health in the US: Dealing with Chronic Back Pain
Back pain hits hard in the US. It costs over $100 billion a year in health care, matching spending on cancer or diabetes (NCBI, 2023). Most cases are due to muscle strains, but others are due to disc problems, arthritis, or stenosis. Pain can be sharp, dull, or burning, and it often limits daily life. For adults over 50, risks rise with age, poor sleep, or extra weight (NCOA, n.d.). Bad sleep worsens pain by boosting inflammation and slowing healing.
People often inquire about treatment options, specifically whether to choose surgery or conservative care. Most start with non-surgical options. These include physical therapy, meds, and lifestyle changes. Surgery is indicated for severe cases, such as when nerves are pinched or there’s weakness (Mayo Clinic Health System, n.d.). Questions to ask your doctor:
What causes my pain?
Do I need imaging tests such as X-rays or MRIs?
What are my options besides surgery?
How long until I feel better?
Conservative care works for many. Exercise strengthens the core, which supports the spine (UC Davis Health, 2025). Quitting smoking helps too, as it harms spinal tissues and raises surgery risks by up to 50% (UMass Memorial Health, n.d.). For long-term relief, prioritize weight control and daily physical activity. This cuts costs, as back pain leads to high medical bills.
Back Health in El Paso, Texas: Local Issues and Choices
In El Paso, back pain is often associated with active lifestyles, factory work, or long drives. Sciatica is common, characterized by radiating leg pain due to nerve compression. It affects the legs, causing numbness or weakness (EP Manual Physical Therapy, n.d.). Spinal stenosis, a narrowing of the spinal canal, causes cramping or tingling that worsens with walking. Herniated discs, bulges, and compressed nerves, leading to pain that’s hard to ignore (Chiro Desert, n.d.). Accidents compound this, with injuries accumulating over time.
People here ask about chiropractic vs. orthopedic surgery. Chiropractors use adjustments to align the spine and relieve pressure, without medication or incision (Bone & Joint, n.d.). They are used to treat mild to moderate pain resulting from strains or poor posture. Orthopedists manage severe cases, such as those requiring surgery for stenosis or disc disease. They use scans and may do injections or fusions (Monitto Chiro, n.d.). Choose based on your issue: chiropractic for non-invasive relief, surgery if nerves are at risk.
Dr. Alexander Jimenez, a local expert in El Paso, notes that back pain often links to inflammation or imbalances. He employs integrative care, including adjustments and nutrition, to address root causes (Dr. Alex Jimenez, n.d.). For sciatica, he suggests checking for gut issues or metabolic problems. His approach is effective for treating accident-related injuries, using X-rays and exercises for recovery. Patients experience less pain and improved mobility with his plans.
For herniated discs or sciatica:
Try decompression: It stretches the spine to retract discs and boost healing (Right Way Chiro, n.d.).
Avoid hazardous movements: Skip back bends or heavy lifts with stenosis (Orthobiologics Associates, n.d.).
See a pro: If pain lasts weeks or causes leg weakness, get checked.
Costs matter in El Paso. Chiropractic visits cost $50- $ 200 and are often covered by insurance, such as Medicare (Healthgrades, n.d.). Check your plan for limits.
Everyday Changes to Avoid Injury and Get Relief
Small habits prevent back pain. Stay active with low-impact activities such as swimming or walking. Strengthen your core for spine support (My Spine Doc, 2026). Good posture cuts strain: Sit with feet flat, screen at eye level.
Tips for daily life:
At work: Use lumbar support, stand every hour, and wear comfortable shoes.
Lifting: Bend knees; keep items close, and do not twist.
Sleep: Side position with knees bent eases stenosis.
Diet: Calcium and vitamin D build strong bones (Jefferson Health, n.d.).
For relief, try ice or heat, stretches, or over-the-counter meds. If pain spreads or includes numbness, see a doctor (Nebraska Medicine, n.d.). In the long term, these changes reduce care costs and improve quality of life.
In the US and El Paso, back health means knowing risks and acting early. Put prevention first with everything from treatment picks to safe backpacks. Consult professionals like Dr. Jimenez for tailored advice. With appropriate steps, most find relief and remain active.
Understand the significance of peptide delivery in buccal absorption physiology and discover its clinical applications.
Abstract
As a clinician deeply engaged in musculoskeletal health, metabolic optimization, and functional neurology, I continually seek delivery systems that are safe, effective, predictable, and clinically practical. Today, I’m presenting an educational overview of modern needle-free peptide delivery via buccal absorption—an approach that aims to make bioactive peptides as accessible as multivitamins while honoring the rigorous standards of clinical pharmacology and physiology. This post draws upon the latest insights from leading researchers and translational scientists working at the intersection of advanced formulation science and functional medicine. It reflects real-world clinical perspectives, pharmacokinetic (PK) findings, and the lived experiences of patients integrating peptides for recovery, inflammation management, immune modulation, and performance optimization.
In this comprehensive exploration, I discuss how dissolvable oral strips—engineered with natural polymers and carbohydrate-based molecular “hubs”—can adhere to the oral mucosa and deliver active substances directly to systemic circulation via microcapillary networks. We will dive into the anatomy of the oral mucosa, including the sublingual, buccal, and palatal regions, and explain how carefully formulated strips use specific adhesion, complexation, and penetration strategies to facilitate rapid uptake while bypassing first-pass hepatic metabolism. We will examine why certain polymers (e.g., pullulan, HPMC), gums (e.g., xanthan, acacia), and sweeteners (e.g., rebaudioside, stevia) are chosen for biocompatibility and patient compliance, and we will highlight how cyclodextrins can act as molecular carriers to improve solubility and permeability of sensitive actives. In addition, we’ll consider the role of short peptides (e.g., cell-penetrating peptides such as penetratin) and excipients that transiently modulate mucosal barrier dynamics to enhance transport.
From a clinical standpoint, this post reviews recent PK data showing high bioavailability with buccal delivery and describes practical use cases, including pain modulation with BPC-157, targeted immune support withthymosin alpha-1, and antioxidant replenishment with glutathione/NAC combinations. We will consider dose-adjustment principles based on body mass, redox status, inflammatory load, and metabolic stress, and discuss strategies for patient selection, monitoring, and compliance. We will also evaluate scenarios wherein injections remain essential, recognizing that needle-free buccal delivery is not a universal replacement but rather a powerful adjunct or alternative within modern integrative care.
Further, we’ll walk through a complex neurological case involving relapsing-remitting multiple sclerosis (MS) to illustrate the interplay of gut-brain-immune systems, the importance of carefully titrated peptide protocols, and the value of objective and subjective outcome tracking. Finally, we will cover practical implementation: patient education, dosing charts, adherence tips, and clinic workflows that reduce repetition and streamline care.
This educational resource is designed to help clinicians and informed patients understand the “why” behind needle-free peptide delivery—its physiological foundations, formulation logic, and clinical utility. As always, the content herein is for educational purposes only; it is not medical advice. Every individual must seek personalized recommendations from their own licensed medical provider. My aim is to illuminate a rapidly evolving area with scientifically grounded, patient-centered context so we can expand access, enhance predictability, and support meaningful health outcomes with modern, evidence-based methods.
Needle-Free Peptide Delivery: Why Buccal Strips Are Changing Patient Care
In my practice, I routinely meet patients who are highly motivated yet constrained by needle aversion, gastrointestinal intolerance, or pill fatigue. Over the last several years, I have observed a meaningful shift toward buccal delivery as a patient-friendly route that supports better compliance, faster onset, and greater predictability—particularly for actives prone to degradation in the GI tract. The concept is simple: use the mouth’s richly vascularized mucosa to deliver actives directly into the systemic circulation, bypassing first-pass metabolism in the stomach and liver, thereby reducing variability and accelerating effects.
The innovation lies not merely in dissolving a compound in the mouth, but in the precise engineering of strips that adhere, stabilize, complex, and permeabilize—briefly and safely—the mucosal barrier for controlled transfer of active pharmaceutical ingredients (APIs) or nutraceutical compounds. The clinical logic is compelling for peptides and other sensitive molecules: many are proteolysis-prone when swallowed; their therapeutic integrity is compromised by gastric and intestinal enzymes (e.g., pepsin, trypsin, chymotrypsin) and pH extremes. Buccal delivery bypasses these degradative steps.
While injections remain highly effective—with subcutaneous delivery typically providing robust bioavailability—needle-free strips offer a complementary option that increases access for those reluctant or unable to use needles and for those seeking a practical option for maintenance therapy, travel, or everyday use. From a clinician’s perspective, having multiple delivery routes increases flexibility in designing personalized protocols that match medical needs and patient preferences.
The Oral Mucosa: A Physiological Highway for Rapid Uptake
The Anatomy and Microvasculature of Oral Absorption
The mouth is more than a gateway for food; it is a finely tuned interface with remarkable microcapillary networks and distinct epithelial regions. The three primary zones relevant to rapid absorption are:
Sublingual space: Under the tongue, with thin, non-keratinized epithelium and rich capillary density, making it ideal for fast uptake of small molecules and certain complexed actives.
Buccal lining: Between the cheek and gum, featuring moderately permeable, non-keratinized stratified squamous epithelium—offering a larger surface area and a more controlled dissolution environment.
Palatal (upper palate) region: The roof of the mouth includes areas of non-keratinized and keratinized epithelium; when strips adhere to the upper palate, saliva flow and tongue pressure can facilitate consistent contact, enhancing mucosal engagement.
Physiologically, the oral mucosa is designed to resist continuous mechanical stress and maintain a barrier against microorganisms, yet it is sufficiently permeable for certain hydrophilic molecules when aided by formulation strategies. Paracellular transport between epithelial cells is limited, but transcellular uptake can be supported through transient modulation of lipid bilayer fluidity, tight junction dynamics, and carrier-mediated mechanisms. The goal is short-lived, reversible permeation that allows actives to traverse into the local capillaries without compromising mucosal integrity or causing irritation.
Bypassing First-Pass Metabolism: Why This Matters Clinically
When a compound is ingested and absorbed through the GI tract, it typically enters the portal circulation and passes through the liver before reaching systemic circulation—a process known as first-pass metabolism. While beneficial for detoxifying exogenous compounds, this pathway can dramatically reduce the bioavailability of certain actives, especially peptides, which are enzymatically cleaved in the GI lumen and enterocytes. By delivering actives via the oral mucosa, we sidestep the gastrointestinal enzymatic gauntlet and the hepatic first-pass filter, often yielding faster and more consistent Cmax (peak plasma concentration) and Tmax (time to peak) profiles.
Clinically, this translates into:
Faster onset of action—critical for sleep initiation compounds, analgesic peptides, or performance-oriented actives.
Lower dose requirements in some cases, because less is lost to metabolism.
Improved predictability—reducing variability due to gut motility, pH, enzyme expression, and microbiome influences.
Enhanced patient adherence—especially in those with pill fatigue or needle aversion.
Modern Buccal Strip Engineering: Adhesion, Complexation, and Permeation
Adhesion: Making Strips Stay Where They Should
A persistent challenge has been ensuring that a strip adheres to the desired mucosal surface long enough for efficient transfer, typically 20–40 seconds or more. Poorly formulated strips tend to slide, fold, or ball up due to tongue motion and saliva, leading to swallowing and reduced efficacy.
Modern strips leverage natural, patient-friendly polymers and gums to achieve controlled mucoadhesion:
Pullulan: A natural polysaccharide with film-forming capacity, offering a smooth mouthfeel and compatible adhesion properties.
Hydroxypropyl methylcellulose (HPMC): A cellulose derivative that stabilizes films and modulates dissolution kinetics.
Gums (e.g., xanthan gum, acacia gum): Used in small amounts to tweak viscosity, flexibility, and adherence.
Natural sweeteners (e.g., rebaudioside, stevia) promote patient acceptance without relying on polyethylene glycols or synthetic flavors that may raise biocompatibility or compliance concerns.
The engineering focus is achieving a balance: sufficient stickiness to maintain contact and resist saliva washout, yet gentle enough to avoid mucosal irritation.
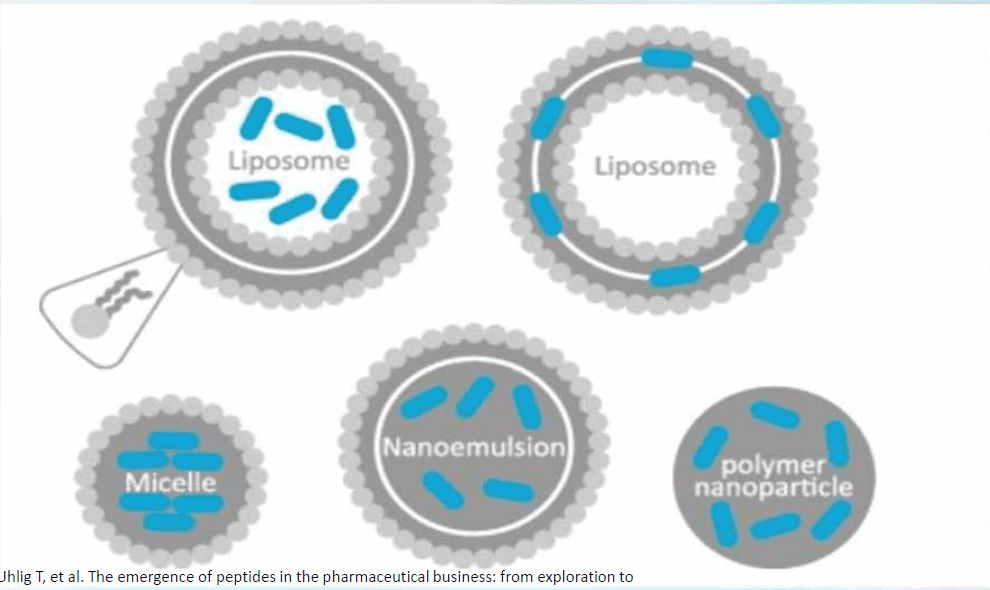
Molecular “Hubs”: Cyclodextrins and Carbohydrate Complexes
To efficiently deliver actives across the mucosal barrier, formulators employ cyclodextrins—cyclic oligosaccharides with hydrophilic outer surfaces and hydrophobic inner cavities that encapsulate lipophilic portions of molecules. This host-guest complexation improves the apparent solubility and stability of sensitive actives, may reduce local irritation, and can “escort” molecules across the mucosa.
Key benefits of cyclodextrin complexes include:
Increased solubility for hydrophobic or amphipathic actives.
Protection from degradation or precipitation within saliva.
Improved interaction with mucosal surfaces, enhancing partitioning into epithelial layers.
Potentially smoother pharmacokinetics due to reduced variability in local dissolution.
Carbohydrate carriers also exploit the mouth’s robust absorption of simple sugars. With salivary amylase initiating carbohydrate breakdown, the environment is well-suited to carbohydrate-based complexes that present activities in forms the mucosa can accommodate.
Short peptides known as cell-penetrating peptides (CPPs)—for example, penetratin—have been explored for enhancing translocation across biological membranes. In carefully controlled doses and time windows, these excipients can transiently soften or modulate mucosal barriers, enabling actives to pass without causing lasting disruption or damage.
Important considerations:
The permeation window should be brief and reversible.
Doses must be carefully controlled to avoid irritation or overexposure.
The aim is to enhance transcellular uptake while respecting barrier function and patient comfort.
Clinical relevance: This targeted, short-lived modulation can achieve faster, more robust Cmax without resorting to aggressive excipients or invasive delivery.
Pharmacokinetics and Bioavailability: How Buccal Strips Perform
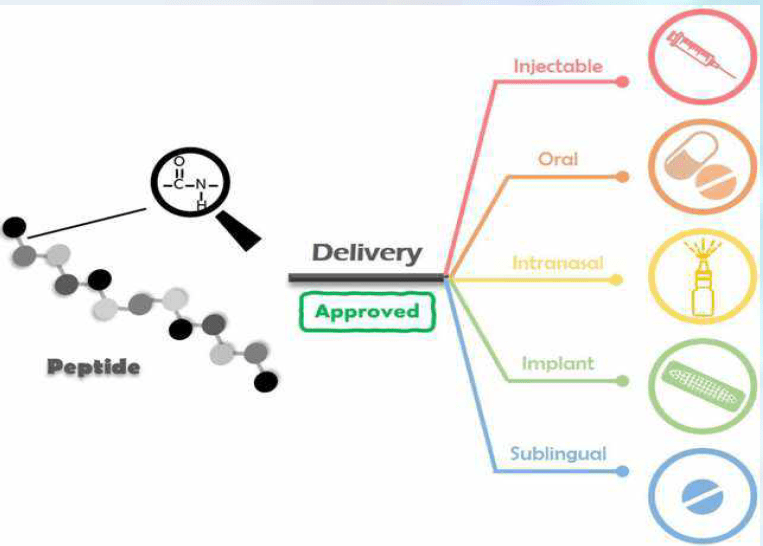
Comparing Delivery Routes: Injection, Oral Ingestion, and Buccal Strips
Every delivery route has merits and limitations:
Subcutaneous injections: High bioavailability (often 80–90%+), direct systemic entry, and reliable kinetics. Limitations include needle aversion, logistics of sterile technique, and local site reactions.
Oral ingestion (capsules/tablets): Convenient, familiar, but for peptides, often compromised by GI proteolysis and first-pass metabolism—resulting in poor or highly variable bioavailability.
Buccal strips: Non-invasive, rapid absorption via mucosa, bypass first-pass effects, and high patient acceptance. In clinical and PK testing, well-engineered strips have demonstrated high bioavailability and predictable uptake profiles.
Recent PK studies of properly formulated buccal strips have shown:
Rapid rise in plasma levels with early sampling times (e.g., 10–30 minutes).
Increased Cmax relative to non-enhanced strips.
Efficient maintenance of circulating reduced glutathione when using antioxidant-focused strips.
Overall, high bioavailability approximating or exceeding that of some subcutaneous routes, depending on the molecule and formulation.
Clinical takeaway: For select actives, particularly sensitive peptides and redox agents, buccal strips can provide a highly effective, patient-friendly alternative to injections.
Clinical Rationale: When and Why I Choose Buccal Strips
Patient Compliance and Practicality
A significant proportion of patients—often near 40% in observational clinic cohorts—express needle aversion. Others struggle with swallowing pills, have GI sensitivities, or experience “pill fatigue” due to complex regimens. Buccal strips improve compliance because they are:
Needle-free and pain-free
Easy to use
Fast-acting
Taste-moderated with natural sweeteners
Suitable across ages (including older adults and those with dysphagia)
From a clinician’s standpoint, improved adherence often correlates with better outcomes, fewer interruptions, and smoother protocol execution.
Speed of Onset and Targeting Specific Outcomes
For sleep support (e.g., melatonin-based strips), rapid buccal absorption can produce onset within minutes, aligning kinetics with bedtime routines.
For pain and recovery peptides (e.g., BPC-157), prompt uptake supports timely relief and faster progression through rehabilitation phases.
For immune support (thymosin alpha-1) and antioxidant replenishment (e.g., glutathione/NAC), buccal delivery can enhance consistency and avoid GI confounders that reduce predictability.
Adjunct, Not Replacement: Keeping Injections in the Toolkit
There are instances where injections remain optimal—such as certain dosing strategies, pharmacologic requirements, or clinical contexts where slow depot delivery is desired. My approach is integrative: buccal strips expand options, improve access, and increase the feasibility of long-term adherence; injections remain important for specific protocols, acute phases, or when clinical evidence dictates.
Physiology Deep Dive: How Peptides Behave and Why GI Ingestion Falls Short
Peptide Structure and GI Degradation
Peptides are chains of amino acids linked by peptide bonds. In the GI tract, proteolytic enzymes (pepsin, trypsin, chymotrypsin, carboxypeptidases) systematically degrade these chains into smaller fragments and free amino acids. While those amino acids are useful, they rarely reconstitute into the original bioactive peptide form within the body.
Gastric environment: Low pH denatures proteins/peptides and activates pepsin.
Intestinal lumen: Pancreatic enzymes further degrade peptides; brush-border peptidases finish the process.
Enterocyte transport: Peptides generally cross as di-/tri-peptides via PEPT1 transporters or as free amino acids—altering pharmacology compared to intact peptide administration.
Clinical implication: Swallowed peptides in capsule form are typically not bioavailable in intact form, reducing or eliminating intended systemic effects.
Buccal Pathway Advantages for Peptides
Buccal strips circumvent the GI enzymatic cascade, delivering intact peptide molecules into the bloodstream through mucosal transfer:
Mucosal permeability: Enhanced by formulation strategies.
Cyclodextrin complexation: Protects and escorts peptides across the mucosa.
Transient permeation: Controlled facilitation minimizes degradation and speeds translocation.
Rapid systemic entry: Aligns kinetics with clinical needs for speed and predictability.
For peptides targeting pain modulation, tissue repair, immune signaling, or neuro-endocrine pathways, maintaining structural integrity and achieving consistent plasma exposure are key.
Case-Based Learning: Practical Applications of Buccal Peptide Strips
Musculoskeletal Recovery and Pain: BPC-157
BPC-157—a peptide frequently discussed in recovery and pain contexts—has gained traction due to its potential roles in angiogenesis, fibroblast activity, collagen synthesis, and modulation of local inflammatory signaling. When delivered via buccal strips:
Patients often report faster symptomatic relief than waiting for oral capsules (which degrade) or scheduling injections.
Clinicians can titrate doses based on response, body mass, and injury severity.
Compliance improves, particularly in patients reluctant to self-inject.
Mechanistically, the rationale includes enhanced local tissue signaling through systemic peptide availability, support for microvascular repair, and moderation of neurogenic inflammation, especially around tendons, ligaments, and joint tissues.
Immune Modulation: Thymosin Alpha-1
Thymosin alpha-1 (Tα1) modulates innate and adaptive immunity, enhances T-cell function, and supportsantiviral and anti-inflammatory responses. Clinically:
Buccal delivery offers consistent exposure without GI variability.
Useful in protocols targeting immune dysregulation, recurrent infections, or high inflammatory tone.
May be paired with antioxidant strips to support redox balance during immune activation.
The physiologic rationale is to maintain predictable peptide levels to influence cytokine signaling, antigen presentation, and lymphocyte activity, while minimizing gastrointestinal confounders.
Redox Replenishment: Glutathione/NAC
Glutathione (GSH) is a central intracellular antioxidant. Direct oral GSH is often degraded or poorly absorbed; NAC (N-acetylcysteine) serves as a precursor for GSH synthesis. Buccal strips containing GSH/NAC can:
Elevate the circulating reduced GSH more rapidly.
Provide predictable absorption kinetics (early Tmax, robust Cmax).
Support detoxification pathways, mitochondrial function, and resilience under metabolic stress.
This is particularly relevant in patients facing oxidative burdens from environmental exposures, chronic inflammation, or metabolic disorders.
Balancing Body and Metabolism-Video
Complex Neurological Case: Relapsing-Remitting MS and Buccal Peptide Protocols
A 55-year-old female with relapsing-remitting MS (diagnosed at age 51) presented with initial symptomatology of constipation—a sign that can suggest autonomic dysregulation or neurogenic contributions—followed by tongue tingling, distal paresthesias, gait difficulty, and visual issues impacting daily function. She was on polypharmacy, including chronic acid blockers, frequent bronchodilator use, diabetes medication, and gait-focused MS therapies with limited perceived benefit. Body weight: approximately 290 pounds—a factor in dosing considerations.
Protocol initiation:
BPC-157 via buccal strips, starting at 500 mcg twice daily for 10 days.
Dose adjustment upward for sustained gains, with monitoring of comfort and function.
Next phase:
Addition of thymosin alpha-1 to support immune function and enhance resilience.
Noted improvements in mobility, endurance, and overall function.
Under physician guidance, cautious reduction in select medications (always coordinated, never unilateral cessation).
Observations:
When peptides were paused, symptoms worsened quickly—particularly gait and fatigue.
Resumption improved outcomes, underscoring the role of consistent exposure for ongoing neuro-immune stabilization.
Clinical reflections:
Complex neuro-immune conditions require careful titration, monitoring, and patient-specific adjustments.
Buccal delivery provided predictability and compliance; GI confounders were minimized.
Longitudinal pulsing strategies may be employed to balance efficacy with sensitivity and avoid tolerance.
Dosing, Body Mass, and Individualization
Weight-Based Considerations
Patients with higher body mass may require adjusted dosing to achieve target plasma exposures—especially for peptides with volume of distribution influenced by body composition. Buccal strips facilitate fractional increases without needle burden, and clinicians can:
Start at standard doses (e.g., 250–500 mcg for BPC-157) and titrate.
Incorporate redox support to enhance peptide signaling efficacy in inflamed or oxidatively stressed environments.
Sensitivity and Tolerability
For sensitive individuals:
Use half-strips as needed.
Slow titration, with close monitoring of symptom response and adverse events.
Ensure patient education: position the strip on the upper palate or buccal lining, perform minimal manipulation, and allow natural dissolution.
Practical Use: How to Apply Buccal Strips Correctly
Place the strip on the top of the tongue; gently close the mouth so it adheres to the roof (palate).
Avoid excessive salivation or sucking motions; allow the strip to dissolve quietly in place.
Alternatively, place the strip between the cheek and gum (buccal lining) based on preference.
Typical adherence/dissolution windows: 20–40 seconds or longer, depending on formulation.
Do not eat or drink immediately after application; give several minutes for optimal absorption, unless otherwise directed.
Clinic Implementation: Education, Tools, and Workflow
To streamline adoption and maintain consistency across providers and patients:
Provide dosing charts, stacking protocols, and oral-use tips.
Offer patient-facing brochures and short educational videos (3–5 minutes) to reduce repetitive explanations during visits.
Use structured case packs or standardized bundles for common indications (pain/recovery, sleep, immune support).
Document outcomes with functional metrics (e.g., timed up-and-go, ROM, daily activity logs) and symptom scales (pain scores, fatigue indices).
The Science of Taste, Texture, and Compliance
Taste and mouthfeel matter. Natural sweeteners and gentle flavoring help:
Reduce aversion and improve adherence.
Avoid synthetic excipients that may irritate the mucosa or raise safety concerns.
Align with patient preferences in integrative clinics where “clean-label” formulations carry weight.
By ensuring strips dissolve cleanly and adhere predictably, clinicians reduce frustration, prevent swallowing during dissolution, and enhance overall experience.
Safety Considerations and Quality Control
Select strips from sources with rigorous quality assurance, batch testing, and transparent excipient lists.
Ensure stability of APIs in the film matrix over time; storage conditions may influence potency.
Monitor for mucosal irritation, allergic reactions, or unusual taste changes.
Educate patients on proper use to avoid chewing/swallowing prematurely.
In clinical settings, consider sequencing: for example, administer antioxidant strips before or alongside peptides in patients with high oxidative load to support efficacy and reduce oxidative interference.
When Buccal Strips Excel and When Injections Remain Preferred
Patients with needle aversion, travel constraints, or dysphagia.
Maintenance therapy requires frequent dosing and steady exposure.
Injections remain preferred when:
A depot effect is needed, or precise parenteral pharmacokinetics are required.
Specific peptides or biologics are unsuitable for mucosal delivery.
Clinical evidence or regulatory guidance favors injectable routes for safety/efficacy.
A flexible, patient-centered approach that leverages both routes yields the best outcomes.
Business and Operational Perspective: Access Without Compromise
Adopting buccal strips can strengthen clinic operations:
Increased adherence reduces protocol failures and the need for repeat explanations.
Predictable absorption improves clinical confidence and efficiency.
Product bundles with dosing guidance simplify onboarding patients.
Practical, needle-free formats enable broader outreach and accessibility.
While business metrics (e.g., margins) matter for sustainability, clinical integrity must define product selection, patient education, and follow-up protocols.
Patient Stories: Translating Science Into Daily Wins
A high-functioning professional with chronic tendinopathy achieves faster rehab milestones with BPC-157 strips, avoiding interruptions from business travel.
An older adult with pill fatigue and mild dysphagia adheres to antioxidant and immune-support strips, stabilizing energy and resilience.
A patient with sleep latency issues benefits from melatonin-containing strips, aligning the onset with sleep hygiene routines in minutes.
These stories illustrate how thoughtful delivery formats make science accessible and actionable.
Research Methods and Evidence-Based Practice
This educational post highlights PK findings, physiologic rationale, and clinical observations drawn from modern formulation research and real-world clinical integration. In the PK context:
Double-blind, controlled comparisons clarify the added value of adhesion, complexation, and permeation strategies.
Early time-point sampling (e.g., 10, 30, 60, 120 minutes) provides meaningful insight into absorption speed and peak exposure.
Maintenance of reduced glutathione indicates functional relevance beyond raw concentration curves.
Even as buccal strips show exceptional promise, we still need robust, peer-reviewed, and replicated studies across diverse molecules, dosing schemes, and patient populations.
Implementation Tips: Training and Support
Train clinicians and staff on placement technique, timing, and counseling.
Provide concise patient materials: one-page instructions plus brief videos.
Create checklists for follow-ups: symptom scores, functional measures, and adverse events monitoring.
Establish clear escalation pathways for dose adjustments and protocol changes.
Consistency in education and monitoring is essential to harnessing the full potential of buccal strips.
Ethical and Regulatory Considerations
Ensure peptides are sourced legally and appropriately for clinical use.
Respect state and national scope-of-practice limitations for prescribing or dispensing.
Maintain documentation of informed consent and rationale for delivery route selection.
Monitor for evolving regulatory guidance on peptide use and mucosal delivery systems.
The goal is responsible integration that prioritizes patient safety and the validity of outcomes.
Advanced Topics: Formulation Nuances and Future Directions
Investigating nanocomplexes within strips to further enhance permeability for larger peptides.
Exploring enzyme-inhibiting excipients that protect peptides locally without systemic effects.
Optimizing hydration layers and film microstructure for even dissolution and contact.
Developing tailored strips for niche indications: neuropeptide support, glymphatic modulation adjuncts, or metabolic signaling peptides.
As formulation science advances, we expect even greater specificity and efficiency in buccal peptide delivery—always guided by clinical outcomes and safety.
Sleep hygiene: time strips with bedtime routines to support sleep-related protocols.
Physical therapy: using recovery peptides alongside graded movement and load management.
Stress modulation: supporting adrenal balance and autonomic regulation.
Environmental health: addressing exposures that drive oxidative stress and immune overactivation.
Multimodal care enhances peptide efficacy and sustains long-term improvements.
Professional Collaboration and Education
Clinicians benefit from sharing case insights, dosing innovations, and adverse event data:
Peer networks and case conferences.
Continuing education on pharmacokinetics and mucosal delivery science.
Joint protocols with physical therapists, nutritionists, and mental health practitioners.
Transparent communication with patients about expectations and evidence status.
The success of needle-free peptide delivery hinges on collective learning and disciplined implementation.
Summary
Buccal peptide strips represent an evidence-informed, patient-centered evolution in peptide delivery. By leveraging oral mucosa physiology and modern formulation strategies—adhesion, cyclodextrin complexation, and transient permeation—these strips achieve rapid, predictable absorption while bypassing the GI tract and hepatic first-pass metabolism. Clinically, they enhance adherence, provide faster onset, and enable flexible dosing without needles.
Key applications include pain and recovery with BPC-157, immune modulation with thymosin alpha-1, and antioxidant replenishment via glutathione/NAC. Case experiences, including complex neurological presentations, demonstrate the practical benefits of consistent buccal delivery and highlight the need for individualized dosing based on body mass, redox state, and clinical goals.
Implementation requires patient education, dosing charts, workflow integration, and monitoring. While injections still play a vital role in certain contexts, buccal strips broaden access and create new care pathways that align with modern evidence and patient preferences.
Conclusion
As a clinician, I value therapies that combine scientific rigor, physiological wisdom, and real-world practicality. Buccal peptide strips embody this triad by transforming how sensitive actives are delivered, making powerful tools accessible to patients who might otherwise be excluded due to needle aversion or GI limitations. The pharmacokinetic data and clinical observations indicate that well-formulated strips can approach or match injection-like bioavailability for select molecules, with remarkable speed and predictability.
The future of peptide therapy is not a single route but a flexible, multimodal ecosystem where injections, buccal strips, and other innovations coexist. Appropriate selection, careful dosing, and thoughtful monitoring are the pillars of safe, effective integration. By continuing to elevate evidence standards and patient education, we can harness buccal delivery to improve outcomes, enhance adherence, and expand access across diverse clinical scenarios.
Key Insights
Buccal strips leverage the mouth’s microcapillary networks to deliver peptides directly into systemic circulation, bypassing GI degradation and first-pass metabolism.
Modern strips use natural polymers, cyclodextrins, and transient permeation strategies to achieve strong mucoadhesion, improved solubility, and rapid, reversible barrier modulation.
Clinical PK data support high bioavailability and fast onset, enabling practical use for pain, recovery, immune modulation, and antioxidant replenishment.
Patient adherence improves dramatically with needle-free formats, reducing pill fatigue and accommodating those with dysphagia or needle aversion.
Injections remain valuable and are not replaced; buccal delivery is a robust adjunct that expands clinical options.
Protocol design must consider body mass, redox status, sensitivity, and functional goals, with patient education and consistent monitoring central to success.
References
Illum L. Mucoadhesive drug delivery systems: characteristics and future promises. Drug Dev Ind Pharm.
Duchêne D, Ponchel G. Bioadhesion of solid oral dosage forms. J Control Release.
Loftsson T, Brewster ME. Pharmaceutical applications of cyclodextrins. Drug solubilization and stabilization. J Pharm Sci.
Mitragotri S, Burke PA, Langer R. Overcoming the challenges in administering biopharmaceuticals: formulation and delivery strategies. Nat Rev Drug Discov.
Pather SI et al. Transmucosal drug delivery: evaluation of mucoadhesive films and tablets. Int J Pharm.
Bruschi ML. Strategies to modify the drug release from mucoadhesive dosage forms. Expert Opin Drug Deliv.
Gallo M et al. Buccal drug delivery: a comprehensive review. Int J Pharm.
Rautio J et al. Prodrug approaches for improving peptide and protein drug delivery. Adv Drug Deliv Rev.
Falco A et al. Cell-penetrating peptides as enhancers of buccal drug delivery: mechanisms and safety considerations. Pharm Res.
Zhuang P et al. Pharmacokinetics of glutathione and NAC via transmucosal administration: implications for redox therapeutics. Front Pharmacol.
Note: References are provided for educational context; clinicians should consult peer-reviewed sources and product-specific data for definitive guidance.
Discover the role of peptide therapies for circadian health plays in achieving better sleep and regulating your body clock.
Hello, I am Dr. Jimenez, and I am delighted to share some insights from my clinical practice and the cutting-edge world of peptide therapy. As a healthcare professional with a dual background as a Doctor of Chiropractic (DC) and a Family Nurse Practitioner (FNP-APRN), I have dedicated my career to integrating diverse medical disciplines to offer holistic, evidence-based care. My focus is on leveraging the body’s innate healing mechanisms, and one of the most powerful tools in this endeavor is the strategic use of peptides to optimize our foundational biological processes. Today, I want to guide you through a key area of health: the intricate relationship among circadian rhythm, restorative sleep, and neurological function. We will explore how modern peptide therapies, grounded in rigorous scientific research, can provide targeted support for these systems, offering hope and tangible solutions for conditions ranging from chronic sleep disturbances and mood disorders to neurodegenerative diseases.
In this educational post, we will explore the science of sleep and biological timing. We will begin by explaining that restorative sleep is not merely a period of rest but a critical, active process for systemic detoxification, hormonal regulation, and cognitive maintenance. I’ll explain the concept of the glymphatic system, the brain’s unique waste-clearance pathway, and how its function is profoundly dependent on the quality of our sleep. We will then turn to the core of our discussion: the role of specific peptides in modulating these processes. I will introduce you to Vasoactive Intestinal Peptide (VIP), a powerful neuropeptide that serves as a master regulator of our circadian clock. We will examine its multifaceted physiological actions, from synchronizing our internal rhythms and promoting the relaxation of smooth muscle in our airways and blood vessels to its significant anti-inflammatory and immune-modulatory effects. I’ll share research demonstrating how intranasal VIP can directly influence the suprachiasmatic nucleus (SCN)—the brain’s master clock—and its cascading benefits for organ systems throughout the body.
Following our exploration of VIP, we will pivot to another groundbreaking area: peptides for mental and cognitive health. I will present a synthetic peptide, PE-22-28, a novel compound with strong potential for treating depression and neurodegenerative conditions. We will delve into its mechanism of action, focusing on its role as a TREK-1 potassium channel antagonist. I’ll explain how, by targeting specific brain regions such as the amygdala and hippocampus, PE-22-28 can exert rapid-acting antidepressant effects, often within days, without the common side effects associated with traditional pharmaceuticals. Furthermore, we’ll examine its neurogenic properties, highlighting research suggesting it can stimulate the growth of new neurons, offering potential therapeutic avenues for conditions such as Alzheimer’s disease, dementia, and cognitive decline.
Finally, we will broaden our scope to discuss other synergistic peptides, such as Oxytocin and DSIP (Delta Sleep-Inducing Peptide), as well as a new combination, Sleeptide. I’ll explain how Oxytocin, often called the “love hormone,” can have surprising benefits for weight management and mood when used correctly. We will also discuss practical clinical applications, including dosing strategies, delivery methods such as intranasal sprays, and the importance of a holistic approach that integrates diet, lifestyle, and targeted supplementation. Throughout this discussion, my goal is to present this information not as a mere lecture but as a comprehensive narrative that illuminates the elegant physiology behind these therapies. By showcasing the work of leading researchers and their modern, evidence-based methods, I aim to empower you with a deeper understanding of how we can harness the power of peptides to reclaim our health, starting with the very foundation of our well-being: a good night’s sleep.
The Critical Role of Restorative Sleep in Systemic Detoxification
As a clinician, one of the first questions I ask my patients, regardless of their chief complaint, is about their sleep. The quality and duration of our sleep are not just lifestyle factors; they are foundational pillars of health. One of the most critical processes that occurs during deep, restorative sleep is systemic detoxification. I often frame it this way to my patients: “I try to optimize the body’s ability to detoxify during its comfort sleep.” This isn’t just a turn of phrase; it’s a physiological imperative.
During our waking hours, our bodies are in a state of high metabolic activity. Our cells produce energy, our muscles contract, and our brains process information; all of these activities generate metabolic byproducts. Think of it as a busy city operating during the day—traffic is high, factories are running, and waste is accumulating. When night falls, and the city sleeps, the cleanup crews come out. In our bodies, this “cleanup crew” is most effective during the deep stages of sleep.
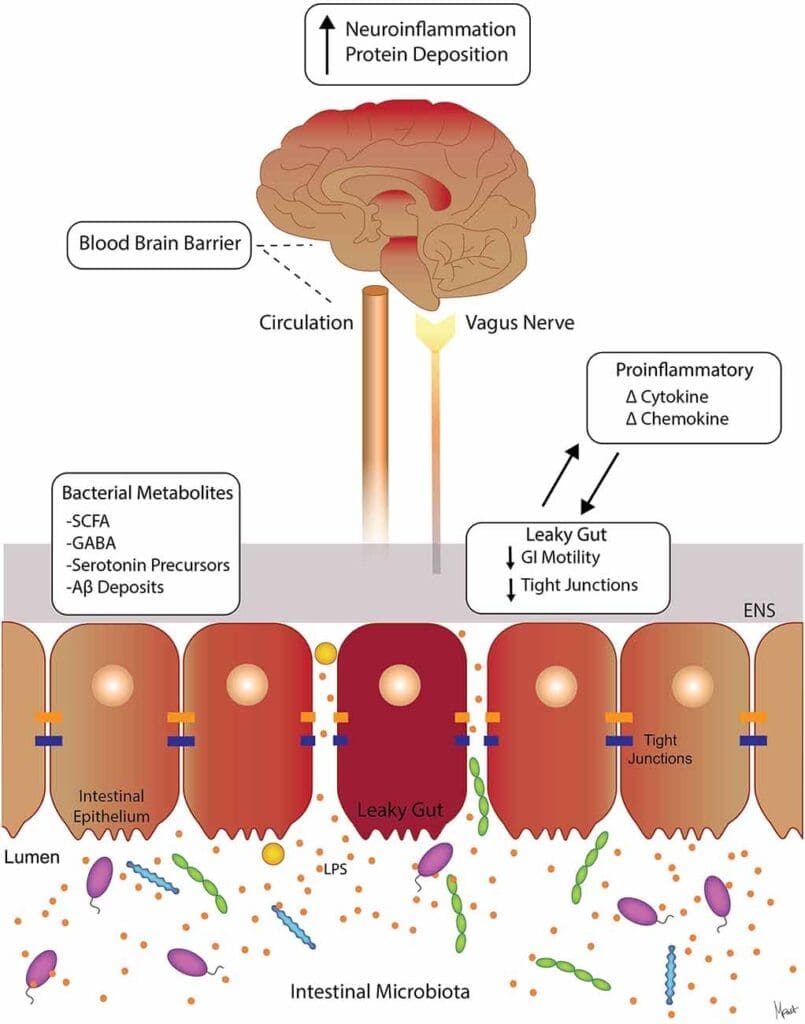
A key player in this process, especially within the central nervous system, is the glymphatic system. This is a relatively recent discovery that has revolutionized our understanding of brain health. Unlike the rest of the body, which has a dedicated lymphatic system to drain cellular waste, the brain was long thought to lack such a network. We now know it has a distinct waste-clearance pathway. The glymphatic system utilizes the cerebrospinal fluid (CSF) that surrounds the brain and spinal cord. During deep sleep, the interstitial space between brain cells actually expands, allowing CSF to flow more freely through the brain tissue, washing away metabolic waste products that have accumulated during the day.
Among the most important of these waste products are amyloid-beta and tau proteins. You may recognize these names, as their accumulation is a hallmark of Alzheimer’s disease and other neurodegenerative conditions. In a healthy, well-slept brain, the glymphatic system efficiently clears these proteins, preventing them from clumping together to form the toxic plaques and tangles that damage neurons. However, when sleep is chronically disrupted or insufficient, this clearance process is impaired. The waste builds up, neuroinflammation increases, and the risk for cognitive decline and dementia skyrockets. This is why a single night of poor sleep can leave you feeling foggy and unfocused, and why chronic sleep deprivation has such devastating long-term consequences for brain health.
My clinical events and observations vary from patient to patient, but the underlying principle remains constant: optimizing sleep is paramount for health and recovery. The strategies we employ to achieve this are highly personalized and often involve addressing the root causes of sleep disruption. This brings us to the master regulator of our sleep-wake cycle: the circadian rhythm.
Vasoactive Intestinal Peptide (VIP): The Master Regulator of Circadian Rhythm
When we talk about synchronizing our body’s internal clocks, few molecules are as influential as Vasoactive Intestinal Peptide (VIP). While many people associate peptides with muscle growth or anti-aging, VIP is a powerful neuropeptide that acts as a master signaling molecule within the brain’s central clock. Its name is somewhat misleading: although it was first discovered in the gut and has effects there, its role in the central nervous system is profoundly important.
I am a strong advocate for maintaining healthy VIP levels and function. From a therapeutic standpoint, my preferred way to modulate its activity is often intranasal administration, sometimes in thermally activated gels that enable sustained release. The intranasal route provides direct access to the brain via the olfactory and trigeminal nerves, bypassing the blood-brain barrier and delivering the peptide to the target site. This isn’t just about facilitating detoxification; it’s about resetting the entire orchestra of our biological rhythms.
A remarkable characteristic of VIP is its longevity in the immune system. Research has shown that its signaling effects can persist for 24 to 72 hours, making it an incredibly efficient molecule for maintaining systemic balance. This sustained action makes it an exceptional peptide for restoring circadian homeostasis.
The Physiology of VIP and the Suprachiasmatic Nucleus (SCN)
To understand VIP’s power, we must look at the suprachiasmatic nucleus (SCN), a tiny region in the hypothalamus that serves as our body’s master clock. The SCN is a cluster of about 20,000 neurons that receives direct light input from the retinas in our eyes. This light signal is the primary cue that synchronizes our internal clock with the external 24-hour day-night cycle.
The neurons within the SCN communicate to generate a cohesive, rhythmic output. VIP is one of the principal neurotransmitters used for this internal communication. It acts as the “conductor’s baton,” ensuring that all the individual neuronal “musicians” in the SCN are playing in time. This synchronized rhythm from the SCN is then broadcast throughout the body, coordinating the “peripheral clocks” in our organs—the liver, pancreas, heart, and even our muscles.
Here’s how it works:
Morning light exposure stimulates the SCN.
SCN neurons release signaling molecules, including VIP, to synchronize their firing patterns.
The SCN then sends signals via the autonomic nervous system and hormonal pathways (such as cortisol and melatonin) to the rest of the body.
These signals tell the liver when to ramp up metabolic enzymes, the pancreas when to release insulin, and the gut when to increase motility.
When this system is working correctly, our body functions like a well-oiled machine. We feel alert during the day and sleepy at night. Our digestion, metabolism, and hormone production are all optimized. However, in modern life, this rhythm is easily disrupted by factors like shift work, late-night screen time (blue light), and irregular eating schedules. This leads to circadian misalignment, a state in which our internal clocks are out of sync with one another and with the external environment. This misalignment is a major driver of chronic disease, including metabolic syndrome, cardiovascular disease, and mood disorders.
A study I often cite in my discussions highlights this mechanism. Researchers demonstrated that VIP is expressed at “super high” levels within the SCN and is indispensable for regulating the circadian rhythm of the central nervous system. When you use VIP, even in a low-dose intranasal spray, you are directly targeting this master clock. You will see profound effects on circadian rhythms not only in the brain but also in other organs that depend on the SCN’s signals.
Systemic Benefits of VIP Beyond the Circadian Rhythm
VIP’s influence extends far beyond timekeeping. It belongs to the secretin/glucagon peptide family, which shares structural similarities and often has overlapping functions. Specifically, the 28-amino-acid peptide VIP shares significant sequence homology with other key signaling molecules, such as PACAP (Pituitary Adenylate Cyclase-Activating Polypeptide). VIP and PACAP often bind to the same receptors (VPAC1, VPAC2, and PAC1), though with different affinities, enabling nuanced and widespread regulatory effects. VIP is present in numerous tissues, including the thyroid, lungs, gut, and immune system, where it exerts a range of vital physiological actions.
Let’s break down some of its key systemic benefits:
Vascular and Muscular Relaxation: VIP is a potent vasodilator, meaning it relaxes the smooth muscle cells lining our blood vessels. This action increases blood flow and helps regulate blood pressure. It also induces non-cholinergic relaxation of vascular and bronchial smooth muscle. This is incredibly important for respiratory health. For patients with conditions like asthma or COPD, where airways are constricted, VIP can be transformative. It will likely relax the airway and reduce inflammation in the airway and pulmonary muscles. This helps to open up the lungs, making breathing easier.
Metabolic Regulation: VIP plays a key role in energy balance. It regulates glycogen metabolism, the process by which our liver and muscles store and release glucose for energy. Promoting glycogen breakdown (glycogenolysis) helps maintain stable blood sugar levels.
Hormonal Regulation: VIP is present in the thyroid gland and helps regulate thyroid hormone secretion. By promoting blood flow to the thyroid and influencing hormone release, it helps to ensure our metabolic rate is properly controlled.
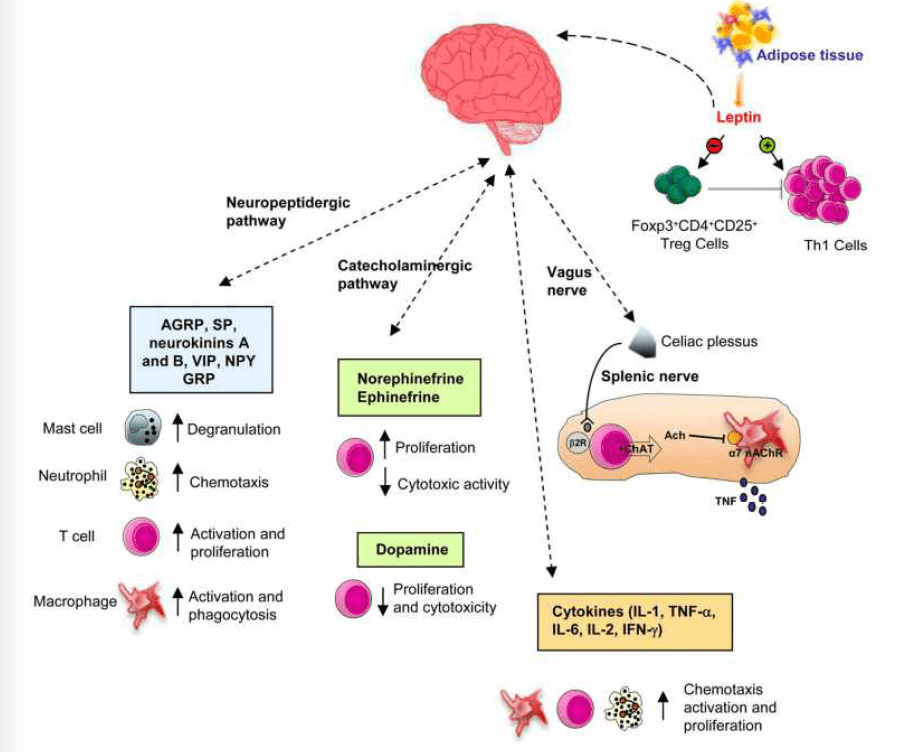
Immune Modulation: This is one of VIP’s most exciting roles. It acts as a powerful anti-inflammatory agent. VIP can suppress the production of pro-inflammatory cytokines while promoting the release of anti-inflammatory ones. It acts as a macrophage deactivating factor, preventing these immune cells from becoming overactive and causing collateral tissue damage. It also helps regulate T-helper cell differentiation, shifting the immune response away from a pro-inflammatory Th1/Th17 profile towards a more tolerant, anti-inflammatory Th2 and regulatory T-cell profile. This makes it a valuable therapeutic candidate for autoimmune conditions and chronic inflammatory states.
Digestive Function: In the gut, VIP regulates intestinal motility, fluid secretion, and blood flow. It helps to relax sphincters and promote the coordinated muscle contractions (peristalsis) that move food through the digestive tract. It also stimulates the secretion of water and electrolytes into the intestine, which is essential for proper digestion and nutrient absorption.
Given this wide range of functions, maintaining optimal VIP signaling is critical to overall health. By using targeted therapies such as intranasal VIP, we are not just helping patients sleep better; we are helping to resynchronize their physiology.
PE-22-28: A Novel Peptide for Rapid Antidepressant Action and Neurogenesis
While restoring sleep is a cornerstone of my practice, I often see patients whose neurological challenges go beyond simple circadian disruption. For those struggling with persistent mood disorders like depression or the cognitive decline associated with neurodegenerative conditions, we need therapies that can directly intervene in the brain’s signaling pathways. I love this particular therapeutic area because when we can help a patient with their mood and memory, we restore their very sense of self. When we’re unable to sleep properly, cognitive deficits and mood instability are among the first to appear, which is why I’m here, exploring these advanced solutions.
One of the most promising agents in this domain is a synthetic peptide called PE-22-28. This is a truly remarkable molecule. PE-22-28 is a synthetic derivative, a fragment of a larger protein, designed to be an antagonist of the TREK-1 potassium channel. To understand why this is so significant, we need to dive into the neurobiology of depression.
The TREK-1 Channel and the Neurobiology of Depression
TREK-1 (TWIK-related K+ channel-1) is a type of potassium channel found on the surface of neurons, particularly in brain regions critical for mood, memory, and emotional regulation. These regions include the amygdala (the brain’s fear and emotion center), the hippocampus (crucial for learning and memory), and the prefrontal cortex.
Potassium channels act as “brakes” for neurons. When they are open, positively charged potassium ions flow out of the neuron, making the cell’s interior more negative (a state called hyperpolarization). This makes it harder for the neuron to fire an electrical signal. In essence, active TREK-1 channels dampen neuronal excitability.
Research in the last decade has strongly implicated the overactivity of TREK-1 channels in the pathophysiology of depression. In animal models of depression, TREK-1 channel expression and activity are significantly increased. This chronic “braking” of neurons in key mood-regulating circuits is thought to contribute to the symptoms of depression, such as anhedonia (the inability to feel pleasure), low motivation, and cognitive impairment.
Traditional antidepressants, like Selective Serotonin Reuptake Inhibitors (SSRIs), work by increasing the levels of neurotransmitters like serotonin in the synapse. While effective for some, they can take weeks or even months to work and come with a host of potential side effects, including emotional blunting, weight gain, and sexual dysfunction.
This is where PE-22-28 comes in. It represents a completely different therapeutic strategy. Instead of indirectly modulating neurotransmitter levels, PE-22-28 directly binds to and blocks the TREK-1 channel. Antagonizing this channel “releases the brakes” on neurons in the amygdala and hippocampus. This increases neuronal firing and plasticity, effectively reversing the cellular state associated with depression.
Rapid-Acting Antidepressant Effects
The most striking finding from research on PE-22-28 is its rapid onset. Studies have shown that it can relieve depressive symptoms in animal models in just four days. This is a monumental leap forward compared to the 4-6 week onset of action for a normal antidepressant.
For a patient in the depths of a major depressive episode, this rapid relief can be life-saving. The clinical protocol I’ve seen emerging from the research involves an initial, more intensive treatment phase. You might start with a dose of intranasal spray three times a day. After four days, once the acute antidepressant effect has been established, the patient can often transition to a maintenance dose, perhaps once daily. The standard starting dose for the nasal spray is typically one spray per nostril. If the patient needs additional support, increase to three to four times daily during the initial phase.
This rapid onset enables a more dynamic and responsive treatment approach. It offers the potential to help patients stabilize quickly, which can be crucial for their safety and overall well-being.
A Favorable Side Effect Profile
Another major advantage of targeting the TREK-1 channel is the potential for a cleaner side effect profile. While the research is still emerging, studies in mice have shown that PE-22-28 does not appear to cause the side effects often associated with other fast-acting antidepressants (like ketamine) or even some conventional medications. For example, some potassium channel modulators have been implicated in seizure activity and cardiac ischemia. However, research in mice shows that none of these side effects were observed with PE-22-28.
This is a critical point for clinicians and patients. Many individuals struggling with depression are also on other medications, and drug interactions are a serious concern. Furthermore, many patients are hesitant to start psychiatric medications due to fear of side effects or dependency. The favorable safety profile of PE-22-28 could make it a much more accessible and tolerable option. If some of your patients are trying to wean off traditional antidepressants, a peptide like this could be particularly effective. Because they do not have the same mechanism of action or dependency profile, they can start treatment with the peptide to achieve stability. Then you can work with them to carefully taper their other psychotropic medications.
Neurogenesis and Cognitive Enhancement
Beyond its antidepressant effects, PE-22-28 has demonstrated potent neurogenic properties. Neurogenesis is the process by which new neurons are generated in the brain. For a long time, it was believed that the adult brain could not create new neurons. We now know this is untrue, and that neurogenesis occurs throughout life, primarily in the hippocampus.
This process is vital for learning, memory, and mood regulation. Interestingly, chronic stress and depression are known to suppress neurogenesis, leading to hippocampal atrophy (shrinkage) and cognitive deficits. Many successful antidepressant therapies, including exercise and SSRIs, are thought to work in part by stimulating neurogenesis.
PE-22-28 appears to be a potent stimulator of this process. Studies show that PE-22-28 not only has effects that are equipotent (of equal strength) to regular antidepressants but also appears to induce neurogenesis with a shorter duration of treatment. In one study investigating neurogenesis in the context of amphetamine use (which can be neurotoxic), PE-22-28 appeared to double the rate of new neuron formation.
This neurogenic capability opens up a vast therapeutic horizon. It means that PE-22-28 may not only alleviate symptoms but also help repair underlying neural damage caused by chronic stress or disease. This is why I use it a lot in my practice for a range of conditions beyond depression:
Alzheimer’s Disease and Dementia: Promoting the growth of new neurons and enhancing synaptic plasticity could help offset the neuronal loss that characterizes these diseases.
Cognitive Decline (“Brain Fog” ): For patients experiencing memory loss or difficulty concentrating, often due to chronic inflammation, hormonal imbalances, or post-viral syndromes, PE-22-28 can help restore cognitive clarity.
Attention-Deficit/Hyperactivity Disorder (ADHD): While more research is needed, its potential to enhance neuronal signaling in the prefrontal cortex could improve executive function and focus.
For my patients, especially the ones who are already working hard on diet and lifestyle but still struggle with memory and cognitive function, this peptide can be a game-changer. It’s important to note that without other supportive interventions—proper nutrition, sleep, and stress management—no single therapy will be a magic bullet. But as part of a comprehensive plan, it will work synergistically with all the other initiatives we are undertaking.
Synergistic Peptides and Holistic Treatment Strategies
While VIP and PE-22-28 are powerful tools, a truly effective clinical approach is rarely about a single molecule. The body is a complex, interconnected system, and the most profound healing often comes from therapies that work in synergy. In my practice, I usually combine these peptides with other agents and lifestyle interventions to create a comprehensive, multi-pronged strategy.
Oxytocin: More Than Just the “Love Hormone”
Another peptide I’d like to mention, even though it wasn’t the focus of the initial transcript, is Oxytocin. Most people know oxytocin as the “love hormone” or “cuddle chemical,” associated with social bonding, childbirth, and lactation. While it certainly does all of those things, its physiological roles are broader, and it can be an effective peptide for a variety of clinical contexts, including weight loss and mood enhancement.
Here’s why:
Anxiolytic and Mood-Elevating Effects: Oxytocin has potent anxiolytic (anti-anxiety) properties. It acts on the amygdala to dampen fear responses and promotes feelings of calm, trust, and well-being. This not only elevates mood but can also indirectly improve sleep by reducing the nighttime anxiety that keeps so many people awake.
Weight Loss and Metabolic Benefits: This is a lesser-known but incredibly important function. Oxytocin has been shown to have anorexigenic effects, meaning it can help to reduce appetite and food intake. It does this by acting on hypothalamic circuits that control satiety. But its real magic for weight loss is in its effect on muscle and fat. Oxytocin supports muscle maintenance during a caloric deficit, which is crucial for maintaining a high metabolism. It also appears to promote the browning of white adipose tissue, converting energy-storing fat into energy-burning fat.
Bone Health: Oxytocin is also effective for conditions such as osteopenia (low bone density). It stimulates the activity of osteoblasts, the cells that build new bone, making it a valuable adjunct for maintaining skeletal health, especially in postmenopausal women.
You can use oxytocin in a troche (a lozenge that dissolves in the mouth) or, my preferred method for systemic effects, as an intranasal spray. It works well for a variety of concerns, but it must be dosed correctly. The patient can use it as a nasal spray, but it is often required to be compounded by a compounding pharmacy to ensure purity and proper concentration.
For weight loss, I often recommend a single spray of intranasal oxytocin after exercise. Using it now capitalizes on the body’s post-exercise metabolic state. It will help preserve muscle while fat is being burned, amplifying the workout’s benefits.
Optimizing Your Wellness- Video
DSIP and Sleeptide: Direct Sleep-Promoting Peptides
For patients whose primary complaint is difficulty initiating or maintaining sleep, we sometimes need peptides that directly promote sleep.
Delta Sleep-Inducing Peptide (DSIP) is a classic in this category. As its name suggests, it was discovered for its ability to promote delta-wave sleep, the deepest and most restorative stage of sleep. We used this one frequently, often via injection. It works by modulating neurotransmitter systems (such as serotonin and GABA) to induce sleepiness.
More recently, new and innovative combinations have emerged. A new product that I like very much is called Sleeptide. This isn’t a single peptide but a proprietary combination of several sleep-promoting peptides and signaling molecules, all within a single delivery system. The idea is that these components will activate upon absorption through the nasal epithelium. It will activate the epithelium’s receptors and deliver a synergistic signal to promote better sleep. The exact formulation of Sleeptide is proprietary to the lab that produces it. Still, it often includes DSIP, a GABA agonist, and other molecules designed to calm the nervous system and promote deep sleep. For patients who have tried single-agent therapies without success, a combination product like Sleeptide can sometimes be the key. It appears to cover more bases by addressing multiple pathways involved in sleep regulation simultaneously.
Integrating Peptides with Lifestyle: The Holistic Approach
It’s crucial to understand that peptides are not a substitute for a healthy lifestyle. They are powerful amplifiers. For any of these therapies to be truly effective, they must be built on a solid foundation of diet, exercise, and stress management, especially for individuals with disrupted circadian rhythms, such as shift workers or new parents.
Let’s consider the example of a shift worker. This person is experiencing forced circadian misalignment. Their SCN is getting light cues at the “wrong” time, and their peripheral organs are constantly struggling to adapt. For these individuals, a peptide like VIP can be highly effective in maintaining some semblance of internal rhythm. However, it must be paired with rigorous lifestyle strategies.
Dietary Timing: This is critical. The timing of meals is a powerful “zeitgeber” (time cue) for our peripheral clocks, especially the liver and pancreas. I work with my patients to establish a consistent eating window, even on workdays. If they work at night, we strategize. Maybe they have their “breakfast” when they wake up in the afternoon and their “dinner” before their shift starts, and then they fast through the night shift. The goal is to keep timing as consistent as possible to avoid sending conflicting signals to the metabolism. We maintain a balanced diet and closely monitor nutrient cofactors.
Nutrient Cofactors: Proper energy metabolism and neurotransmitter synthesis depend on a host of micronutrients. I always look at levels of B vitamins, magnesium, vitamin D, zinc, and selenium. I also frequently check for CoQ10. These are all critical cofactors for mitochondrial function and the proper oxidation of fuels. I often rely on testing for these nutrients at work. I want to understand their status and balance them. If you need to supplement, you supplement. But it must be a targeted approach based on lab work.
Light Environment Control: For shift workers, managing light is everything. This means using bright light therapy upon waking (even if it’s 3 PM) to signal “daytime” to the SCN. It also means wearing blue-light-blocking glasses for the last few hours of their shift and on the commute home to prepare the brain for sleep. Their bedroom must be a veritable cave—blackout curtains, no electronics, cool temperature.
Sleep Consistency: We know there’s no way we can fully adjust to a different schedule every few days. The body is partly hard-wired for a day-active cycle. We can help them establish a routine as consistent as possible. They need to get on a diet that supports their energy needs and aim for a consolidated block of seven or eight hours of sleep, even if it’s during the day. This is the ideal, and while it’s not always achievable, the goal is to find something that allows them to get a solid, uninterrupted sleep block.
Practical Considerations: Dosing, Delivery, and Sourcing
When implementing peptide therapies, the details matter immensely. Dosing, delivery method, and peptide source are critical to safety and efficacy.
Delivery Methods: Why Nasal Sprays?
Throughout this discussion, I’ve frequently mentioned intranasal sprays. There’s a good reason for this. For peptides targeting the central nervous system, this delivery method offers several distinct advantages:
Bypassing the Blood-Brain Barrier (BBB): The BBB is a highly selective membrane that protects the brain from pathogens and toxins. Unfortunately, it also blocks most large molecules, including many peptides, from entering the brain when taken orally or injected systemically. The nasal cavity, however, offers a direct pathway to the brain via the olfactory and trigeminal nerves, allowing peptides to bypass the BBB and reach their targets in the CNS.
Rapid Onset of Action: This direct transport route enables the peptide to reach the brain quickly, resulting in a faster onset of action than oral administration, which requires digestion and first-pass metabolism in the liver.
Ease of Use and Patient Compliance: A nasal spray is non-invasive, painless, and easy for patients to administer themselves at home. This is a huge advantage over therapies that require daily injections, which can be a significant barrier for many people.
That said, other methods, such as subcutaneous injections or oral troches, have their place depending on the peptide and the desired effect.
Dosing and Sourcing: The Importance of Precision
Peptide dosing is highly specific and often measured in micrograms (mcg), not milligrams (mg). This highlights their potency. The correct dose depends on the peptide, the patient’s weight, their condition, and the specific lab that compounded the formula.
VIP: A typical intranasal dose is approximately 50 mcg per spray, used once or twice daily to support circadian rhythm. You can find VIP in various concentrations. Some labs may report 100 mcg/mL, while others report 20 mcg/mL. The nasal sprays I use are typically 50 micrograms per spray and are used once a week for maintenance or more frequently for acute resetting. It varies from patient to patient.
PE-22-28: As discussed, a starting protocol might be one spray per nostril (each spray delivering a specific microgram dose) up to three times daily for the first four days, then taper to a maintenance dose.
Oxytocin: Doses can vary widely. For post-exercise use, one spray in each nostril might be sufficient.
DSIP and Sleeptide: These are typically used only at bedtime.
The most critical factor is the peptide source. Peptides must be sourced from a reputable, licensed compounding pharmacy. I use labs such as Tailor Made Compounding, CRE8 Pharmacy (which I believe ships to every state), and other PCAB-accredited facilities. These pharmacies synthesize peptides under sterile conditions and conduct third-party testing to verify purity, potency, and the absence of contaminants. This is not an area to cut corners. Using peptides from unregulated “research chemical” websites is incredibly dangerous, as you have no guarantee of what you are actually getting.
It’s also important to note that concentrations across labs can vary. A nasal spray from one pharmacy may contain 50 mcg per spray, while another may contain 200 mcg. That’s why working with a knowledgeable provider is essential. They will know the reputable labs and how to convert and prescribe the correct dose based on the specific formulation you are using. The dosages are not like a simple tablet from a conventional pharmacy; they require careful calculation and adjustment.
Summary, Conclusion, and Key Insights
Summary
In this comprehensive overview, I, Dr. Jimenez, have guided you through the advanced use of peptide therapies to optimize sleep, neurological health, and overall well-being. We began by establishing the critical importance of restorative sleep as an active process of systemic detoxification, with a focus on the brain’s glymphatic system and its role in clearing metabolic waste, such as amyloid-beta. We then examined specific peptide interventions, beginning with Vasoactive Intestinal Peptide (VIP). I explained its function as a master regulator of the circadian rhythm by acting on the brain’s suprachiasmatic nucleus (SCN). We explored its diverse physiological benefits, including vasodilation, bronchodilation, immune modulation, and metabolic regulation, highlighting its therapeutic potential when administered intranasally.
Next, we transitioned to the groundbreaking synthetic peptide PE-22-28. I detailed its mechanism as a TREK-1 potassium channel antagonist and how it enables rapid-acting antidepressant effects, often within days. We examined its favorable safety profile and its profound neurogenic properties, which suggest its utility in treating not only depression but also neurodegenerative conditions like Alzheimer’s and cognitive decline. Finally, we discussed the synergistic use of other peptides like Oxytocin, for its mood-enhancing and metabolic benefits, and sleep-promoting agents like DSIP and the combination formula Sleeptide. I emphasized that these powerful tools are most effective when integrated into a holistic framework that includes precise dietary timing, targeted nutritional supplementation, and rigorous lifestyle management, particularly for individuals with disrupted circadian rhythms.
Conclusion
The future of medicine lies in precision and personalization, moving beyond one-size-fits-all approaches to leverage the body’s own intricate signaling systems. Peptide therapy represents a monumental step in this direction. By using molecules that are either identical to or derived from our body’s natural regulators, we can intervene with a level of specificity and elegance that was previously unimaginable. The peptides discussed here—VIP, PE-22-28, and Oxytocin—are not just treating symptoms; they are targeting the root physiological and neurological dysfunctions that underlie conditions ranging from insomnia and depression to cognitive decline. As we continue to unravel the complexities of human physiology, these evidence-based peptide strategies will become increasingly integral to promoting optimal health, restoring function, and enhancing human potential. The key to unlocking this potential lies in a collaborative partnership between an informed patient and a knowledgeable clinician who can safely and effectively navigate this exciting frontier of medicine.
Key Insights
Sleep is an Active Detoxification Process: Deep sleep is essential for the brain’s glymphatic system to clear neurotoxic waste products. Chronic sleep disruption impairs this process, increasing the risk for neurodegenerative diseases.
VIP is a Master Circadian Regulator: Vasoactive Intestinal Peptide (VIP) is a critical neurotransmitter in the brain’s master clock (the SCN). Intranasal VIP therapy can help resynchronize a disrupted circadian rhythm, with cascading benefits for hormonal, metabolic, and immune health.
PE-22-28 Offers Rapid Antidepressant Action: By blocking the TREK-1 potassium channel, the synthetic peptide PE-22-28 can relieve depressive symptoms in as little as four days, offering a rapid and potentially safer alternative to traditional antidepressants.
Neurogenesis is a Target for Cognitive Health: PE-22-28 is a potent stimulator of neurogenesis (the growth of new neurons), making it a promising therapeutic for cognitive decline, dementia, and Alzheimer’s disease.
A Holistic Approach is Essential: Peptide therapies are most effective when used as part of a comprehensive plan that includes lifestyle interventions such as timed eating, light management, and targeted supplementation with key nutrient cofactors (e.g., Vitamin D, Zinc, CoQ10).
Sourcing and Dosing are Critical: The safety and efficacy of peptide therapy depend entirely on using high-purity products from reputable compounding pharmacies and adhering to precise, individualized dosing protocols prescribed by a qualified healthcare provider.
References and Keywords
References:
While this post is a narrative synthesis of clinical knowledge and research findings, the concepts discussed are based on established scientific literature. Interested readers are encouraged to search for primary research articles on platforms like PubMed and Google Scholar using the keywords below. Key research areas include:
Nedergaard, M. (2013). Garbage Truck of the Brain. Science. (On the glymphatic system).
Lande, S., et al. (1971). Isolation of a potent sleep-inducing peptide from rabbit brain. FEBS Letters. (On the discovery of DSIP).
Harmar, A.J., et al. (2012). The VPAC2 Receptor and the Circadian Timing System. British Journal of Pharmacology. (On VIP’s role in the SCN).
Baudry, M., et al. (2017). A Novel Trophic Factor TrkB-Ligand with Antidepressant and Anxiolytic Activities. Molecular Psychiatry. (On the development and mechanism of PE-22-28, also referred to as a TrkB ligand in some literature).
Mazzocchi, G., & Malendowicz, L. K. (2011). Vasoactive intestinal peptide and the thyroid. International Review of Cytology. (On VIP’s role in thyroid function).
Delgado, M., & Ganea, D. (2013). Vasoactive intestinal peptide: a neuropeptide with pleiotropic immune functions. Amino Acids. (On the immunomodulatory effects of VIP).
Lawson, E. A. (2017). The effects of oxytocin on eating behaviour and metabolism in humans. Nature Reviews Endocrinology. (On oxytocin’s role in weight management).
The information provided in this educational post is intended for informational and educational purposes only. It is not intended to be a substitute for professional medical advice, diagnosis, or treatment. The content is written from the perspective of Dr. Jimenez (DC, FNP-APRN) and reflects their clinical experience and interpretation of current research. However, it should not be construed as direct medical advice.
Never disregard professional medical advice or delay in seeking it because of something you have read in this post. Always seek the advice of your own physician or other qualified health provider with any questions you may have regarding a medical condition. Do not start, stop, or change any part of your healthcare plan or treatment without consulting your medical provider. Reliance on any information provided in this post is solely at your own risk.
All individuals must obtain recommendations for their personal situations from their own medical providers. The peptides, protocols, and dosages mentioned are illustrative examples based on emerging research and clinical practice and may not be appropriate for everyone. Self-administering these substances without medical supervision can be dangerous.
A nurse practitioner and a doctor of chiropractic meet with a patient with neuropathy
Neuropathy happens when nerves get damaged. It often causes burning pain, tingling, numbness, or weakness—usually in the feet and hands. Millions deal with this every day, and it can make simple tasks harder. At ChiroMed in El Paso, TX, the team uses an integrated approach to treat root causes rather than just mask symptoms (ChiroMed, n.d.).
Diabetes is the most common cause. High blood sugar harms the tiny blood vessels that feed nerves. Other triggers include injuries, infections, vitamin shortages, chemotherapy, autoimmune issues, or even gluten-related inflammation. While some neuropathy improves when the cause is fixed, diabetic cases often need ongoing management to slow progression and ease pain (HealthCentral, n.d.; ChiroMed, 2025b).
Patients at ChiroMed frequently ask the same questions:
What caused my neuropathy?
What is the best medication for this pain?
Are there non-drug options that really work?
Why does my pain get worse at night?
What if my current treatment isn’t helping?
ChiroMed’s dual-credentialed provider, Dr. Alexander Jimenez, DC, APRN, FNP-BC, answers these directly. As both a Doctor of Chiropractic and board-certified Family Nurse Practitioner, he creates personalized plans that combine medication management with natural therapies.
Common Causes and Early Symptoms of Neuropathy
Diabetes → damages nerves through poor circulation
Injuries or spine issues → compress nerves
Toxins & inflammation → including gluten sensitivity
Vitamin deficiencies → especially B vitamins
Autoimmune or chemotherapy-related damage
Early signs include tingling, burning feet, balance problems, or muscle weakness. Catching it early helps prevent complications such as falls or ulcers (Azar et al., 2020; ChiroMed, 2025a).
Best Medications for Neuropathy Pain
There is no single “best” pill—it depends on your health history. First-line medications that change how pain signals travel include:
Gabapentin → calms overactive nerves; may cause dizziness
Pregabalin → similar to gabapentin; often faster relief
Duloxetine → an SNRI that boosts natural pain-fighting chemicals
These are recommended by guidelines for diabetic and other neuropathies (Attal et al., 2017; NHS, n.d.). At ChiroMed, Dr. Jimenez starts with the lowest effective dose, monitors side effects closely, and adjusts quickly because he holds both NP and chiropractic licenses.
Common side effects to expect:
Mild drowsiness or dizziness
Dry mouth or nausea
Weight changes (especially with pregabalin)
Topical creams, such as lidocaine patches or capsaicin, are also used to relieve localized burning pain.
Why Neuropathy Pain Feels Worse at Night
Pain often spikes at night because:
Fewer distractions let the brain focus on nerve signals
Lying down changes blood flow and nerve pressure
Temperature drops can make symptoms flare
Quick nighttime tips:
Wear soft socks to keep your feet warm
Use white noise or a fan
Elevate feet slightly
Take evening doses of medication if prescribed
Non-Drug Treatments That Work Well
Many patients prefer or need options beyond pills. ChiroMed offers several proven alternatives:
Chiropractic adjustments → improve spinal alignment and blood flow to nerves
Acupuncture → stimulates natural pain relief
Therapeutic exercises & rehabilitation → build strength and balance
Nutrition counseling → target inflammation and vitamin gaps
Cold laser therapy → supports nerve healing
TENS units → gentle electrical stimulation
Dr. Jimenez often uses chiropractic care for diabetic neuropathy and nerve damage linked to gluten sensitivity. These approaches reduce inflammation and enhance nerve function without relying solely on medication (ChiroMed, 2025a; ChiroMed, 2025b).
Additional helpful therapies:
Manual soft-tissue work
Functional movement training
Naturopathic support for blood-sugar balance
What to Do When Medication Isn’t Enough
If pain continues, the next steps include:
Dose adjustment or medication switch
Adding non-drug therapies
Diagnostic testing to rule out new causes
Referral to advanced options like nerve stimulation
ChiroMed’s integrated model shines here—Dr. Jimenez can manage prescriptions as an NP while adding chiropractic and rehab as a DC.
How Nurse Practitioners at ChiroMed Help
Nurse practitioners provide full-scope care: prescribing medications, ordering labs, monitoring progress, and creating custom plans. At ChiroMed, NPs focus on:
Safe medication management
Foot safety education (key to diabetes)
Lifestyle coaching for blood-sugar control
Coordinating with your primary doctor
This whole-person approach improves daily function and reduces complications (Haddad et al., 2021; NurseTogether, n.d.).
Integrative Chiropractic Care at ChiroMed
Chiropractic at ChiroMed goes beyond adjustments. Dr. Alexander Jimenez uses:
Spinal decompression
Targeted rehabilitation
Functional nutrition
Electro-acupuncture
His 30+ years of experience show that combining chiropractic with medical care gives better long-term relief for neuropathy, sciatica, and chronic nerve pain (Jimenez, n.d.a; ChiroMed, n.d.).
Benefits patients notice:
Less burning and tingling
Better balance and walking
Reduced need for high-dose medications
Improved sleep and energy
The Power of Combined NP + Chiropractic Care at ChiroMed
ChiroMed’s unique advantage is having both services under one roof. Dr. Jimenez’s dual training means seamless coordination—no bouncing between offices. Patients get:
Medication when needed
Hands-on nerve relief
Nutrition and rehab support
One personalized treatment plan
This multidisciplinary model has helped thousands in El Paso reduce pain and regain mobility (Progressive Health Clinic, n.d.; ChiroMed testimonials).
Living a Full Life with Neuropathy
Neuropathy doesn’t have to control your days. With the right combination of medications, lifestyle changes, and integrated therapies, most people feel much better. ChiroMed in El Paso specializes in exactly this kind of care.
Practical daily tips:
Walk or swim for gentle exercise
Eat anti-inflammatory foods
Check feet daily
Stay consistent with treatment
Early action makes the biggest difference.
If you’re in El Paso and struggling with neuropathy pain, schedule a consultation at ChiroMed. Call (915) 412-6680 or visit https://chiromed.com/ to meet Dr. Alexander Jimenez and experience integrated relief.
Understand the importance of cellular health and fascia in managing systemic inflammation. Enhance your wellness journey today.
By Dr. Alex Jimenez, DC, FNP-APRN
Introduction: Charting the Course for a Longer, Healthier Life
Welcome to this in-depth exploration of the new frontier in longevity and cellular health. As a practitioner dedicated to both the structural and systemic aspects of human wellness, holding credentials as a Doctor of Chiropractic (DC) and a Family Nurse Practitioner (FNP-APRN), I have always been driven by a singular mission: to integrate the most advanced, evidence-based research into practical, effective clinical strategies. This post is the culmination of that mission, designed to distill complex, cutting-edge science into a clear, actionable framework for health. We are moving beyond the traditional, fragmented view of the body and embracing a holistic, interconnected systems-based approach. We will not be talking in hypotheticals; instead, we will present the latest findings from leading researchers in the field, showcasing their work through modern, evidence-based research methods to illuminate the path toward a longer, more vibrant life.
In the sections that follow, we will embark on a comprehensive journey into the very fabric of our being. We will begin by demystifying the concept of aging itself, reframing it not as an inevitable decline but as a modifiable process rooted in what modern science calls the “Hallmarks of Aging.” A central theme will be the concept of “inflammaging,” the chronic, low-grade inflammation that silently accelerates the aging process and underlies nearly every chronic disease. We will discuss why establishing a baseline of your unique biological data from a young age is no longer a luxury but a necessity for predictive and personalized medicine.
From there, our exploration will dive deep into the fascinating world of the fascial system—the body’s ubiquitous connective tissue network. Once dismissed as mere “packing material,” fascia is now recognized as a primary sensory and communication organ, a “body-wide web” that influences everything from our posture and movement to our immune function and cellular health. We will unpack the intricate physiology of fascia, its relationship with the extracellular matrix (ECM), and the pivotal role of its health in optimal cellular signaling, nutrient exchange, and waste removal. You will learn how the fascial system can become dense and fibrotic due to injury, stress, and inflammation, creating a “cellular prison” that perpetuates dysfunction and pain.
A significant portion of our discussion will focus on the immune system’s intimate relationship with the fascial network and the ECM. We will examine how immune cells, such as macrophages, lymphocytes, and mast cells, reside within and are influenced by this matrix. We will explore the Cell Danger Response (CDR), a universal metabolic response to threat, and how a persistent CDR can lead to chronic inflammation and a breakdown in immune tolerance, setting the stage for autoimmune conditions and accelerated aging. This will lead us to a critical analysis of modern metabolic health, particularly the hidden dangers of hyperinsulinemia and its devastating impact on cellular function, even in individuals with “normal” blood sugar. We’ll present a compelling case for why measuring fasting insulin alongside glucose is a non-negotiable aspect of any true health assessment.
Finally, we will translate this deep physiological understanding into practical, evidence-based interventions. We will critically evaluate therapies such as cryotherapy (cold treatment) and thermotherapy (heat therapy), moving beyond simplistic advice to provide nuanced guidelines for their proper application in acute injury versus chronic remodeling. We will also touch on the powerful potential of targeted interventions such as peptides (e.g., BPC-157) and photobiomodulation (red light therapy) to support tissue repair, modulate the immune system, and restore cellular homeostasis. Throughout this post, my goal is to empower you with knowledge—to help you understand the why behind the what, so you can become a more informed and active participant in your own health journey. This is not about chasing fads; it is about building a foundation of resilient health based on the profound and elegant principles of human physiology.
Redefining Aging: From Inevitability to a Modifiable Process
For centuries, we’ve viewed aging as a one-way street of inevitable decline. However, a seismic shift is occurring in medical science. We are beginning to understand aging not merely as the passage of time, but as a specific, definable biological process characterized by a collection of interconnected dysfunctions known as the “Hallmarks of Aging.” This perspective is revolutionary because it reframes aging as a condition that can be studied, understood, and, most importantly, modified.
The conversation has moved from “how long we live” to “how well we live” for the duration of our lives—our healthspan. The goal is no longer to add years to life, but to add life to our years. This involves actively working to re-function, regenerate, and create resilience within our own biology.
The Critical Importance of a Biological Baseline
One of the most foundational principles of this new paradigm is establishing a biological baseline. Imagine trying to navigate a complex journey without a map or a starting point. That’s precisely what we do when we wait for a disease to manifest before taking a deep look at our health.
When I work with patients, whether they are young children or their aging parents, the first and most crucial step is to capture a comprehensive snapshot of their current physiological state. This isn’t just a standard physical; it’s a deep dive into their molecular and cellular world. This baseline becomes our immutable point of reference.
For example, if a patient comes to me today, in 2024, and we run a comprehensive panel of biomarkers, that data is locked in. If they return in 2026 after experiencing a health challenge or simply as part of a proactive monitoring plan, we don’t have to guess what “normal” looks like for them. We can compare their new results directly to their unique baseline. This allows us to detect subtle shifts and deviations long before they snowball into a full-blown clinical diagnosis. It’s the essence of predictive and preventative medicine.
Ideally, this process should begin in youth. By understanding an individual’s genetic predispositions and establishing their unique physiological “signature” early on, we create a roadmap for a lifetime of personalized health optimization. This is about being in a constant state of readiness. Like a well-prepared military, we aren’t waiting for a crisis to happen; we are building the resources and intelligence to anticipate and mitigate threats before they escalate.
Aging as an Informational Problem: Senescence and Geriatric Genes
At its core, aging can be viewed as an informational problem. Our DNA is the blueprint, but it’s the epigenome—the layer of chemical tags that tells our genes when to turn on and off—that acts as the software. Over time, due to environmental insults, lifestyle factors, and metabolic dysfunction, this “software” can become corrupted.
This leads to a phenomenon called cellular senescence, where cells lose their ability to divide and function properly. These “zombie cells” don’t just sit there quietly; they secrete a cocktail of inflammatory signals known as the Senescence-Associated Secretory Phenotype (SASP), which poisons the surrounding tissue environment and accelerates the aging of neighboring cells.
This is an informational breakdown. The cell’s internal programming has been disrupted. For example, in an aging liver or ovary, the epigenetic signals can begin to turn on what we might call “geriatric genes”—genes that promote fibrosis, inflammation, and a loss of functional capacity. Our goal is to maintain the integrity of that original, youthful genetic “software” for as long as possible. Understanding a person’s baseline is the first step in monitoring and protecting that precious informational code.
The Fascial System: Your Body’s Intelligent, Interconnected Web
If we are to understand health and longevity truly, we must look beyond individual organs and systems and appreciate the tissue that connects them all: fascia. For too long, fascia was dismissed in anatomy labs as the white, fibrous “stuff” that you had to cut through to get to the “important” structures like muscles and organs. Modern research, however, has unveiled fascia as one of the most vital and intelligent systems in the body.
Think of it as a continuous, body-wide tensional network that exists from head to toe, from skin to bone. It’s not just a series of disconnected sheets; it’s a single, uninterrupted web. This web has three main layers:
Superficial Fascia: Located just beneath the skin, rich in fat, nerves, and blood vessels.
Deep Fascia: The dense, fibrous layer that envelops and separates muscles, bones, and organs, forming compartments and transmitting mechanical force.
Visceral Fascia: The layer that surrounds and suspends our organs within their cavities.
But it goes even deeper. Fascia continues into the structures it surrounds. The connective tissue wrapping a muscle (epimysium), a muscle bundle (perimysium), and even a single muscle fiber (endomysium) are all part of this continuous fascial matrix. It even extends to the covering of our nerves (epineurium, perineurium, endoneurium). It is, in every sense, the fabric that holds us together.
Fascia as a Primary Sensory and Communication Organ
Perhaps the most groundbreaking discovery is that fascia are among our richest sensory organs. It is densely populated with mechanoreceptors—nerve endings that sense pressure, tension, and movement. In fact, it’s estimated that the fascial network contains a staggering number of sensory nerve endings, potentially rivaling or even exceeding that of the retina. Some leading researchers, like Dr. Robert Schleip, posit that up to 80% of our interoceptive information—the sense of our body’s internal state—originates from the sensory nerves embedded in our fascia, not just from our muscles.
This has profound implications. When you feel “stiff,” “tight,” or have a poor sense of your body’s position in space, you are receiving signals from your fascial network. This system is constantly communicating with the central nervous system, providing a real-time feedback loop on our mechanical status, hydration levels, and overall physiological well-being. It is the physical substrate of our mind-body connection. Energy and information travel through this network at incredible speed. While we are roughly 70% water by weight, the molecules that make up our bodies are 99% water molecules. This aqueous, crystalline matrix of the fascia is the perfect medium for conducting bioelectric and mechanical signals.
Fascial Lines and the Transmission of Force
Fascia is not arranged randomly. It organizes itself along lines of tension, creating what pioneers like Tom Myers have termed “Anatomy Trains” or myofascial meridians. These are continuous lines of fascial connection that link different parts of thebody.
A classic example is the Superficial Back Line, which runs from the bottom of your feet, up the calves and hamstrings, over the sacrum, up the erector spinae muscles, and over the top of the skull to your eyebrows. This explains why tension in your feet can contribute to headaches, or why tightness in your hamstrings can cause low back pain.
Another crucial line is the Spiral Line, which loops around the body like a double helix, connecting, for example, the left shoulder to the right hip. This is the line that governs rotational movements, like throwing a ball or walking. An imbalance or restriction anywhere along this line will compromise the efficiency and fluidity of the entire chain. This is why a therapist might work on your hip to resolve a shoulder problem—they are not treating the site of pain, but the source of the dysfunction within the interconnected fascial web. This interconnectedness is the very reason why a holistic approach to the body is not just a philosophy, but a physiological necessity.
The Extracellular Matrix (ECM): The Cellular Neighborhood
To understand how fascia influences health at the most fundamental level, we must zoom in from the macroscopic fascial planes to the microscopic environment surrounding every cell in our body: the Extracellular Matrix (ECM). The ECM is the non-cellular component of all tissues. If the cells are the residents of a neighborhood, the ECM is the entire infrastructure—the roads, communication lines, waste-disposal systems, and public parks.
The ECM is a complex, gel-like substance primarily produced and maintained by cells called fibroblasts. It is composed of a rich “cocktail” of molecules, including:
Collagen: The primary structural protein, providing tensile strength and stability. There are many types, with Type I being the most abundant and providing rigidity. At the same time, Type III (reticular collagen) is finer and more flexible, often found in new tissue and during the early stages of wound healing.
Elastin: A protein that allows tissues to stretch and recoil, providing elasticity.
Proteoglycans and Glycosaminoglycans (GAGs): These are large molecules (like hyaluronic acid) that attract and hold vast amounts of water, creating the hydrated, gel-like consistency of the ECM. This hydration is critical for shock absorption and for facilitating the diffusion of nutrients and signaling molecules.
The ECM is not passive scaffolding. It is a dynamic, biologically active environment in constant, bidirectional communication with the cells living within it. Cells use the ECM to impart strength and shape to tissues, but the ECM, in turn, dictates cell behavior. It provides physical and biochemical cues that influence cell differentiation, migration, proliferation, and survival. Hormones, growth factors, and cytokines all travel through and are modulated by the ECM to reach their target cells.
When the Neighborhood Goes Bad: Fibrosis and the Cell Danger Response
In a healthy state, the ECM is a fluid, adaptable, and resilient environment. However, following injury, chronic inflammation, or metabolic stress, this neighborhood can become a very hostile place.
This is where the Cell Danger Response (CDR) comes into play. The CDR, a concept brilliantly articulated by Dr. Robert Naviaux, is a universal, evolutionarily conserved metabolic response that a cell initiates when it perceives a threat—be it a virus, a toxin, or a physical injury. The cell essentially shifts its priorities from “peacetime” functions (growth, repair, social interaction with other cells) to “wartime” functions (defense). It hunkers down, hardens its membrane, and changes its metabolism.
If this threat is acute and resolved quickly, the cell returns to its normal state. But if the danger is chronic—persistent inflammation, ongoing metabolic stress, unresolved emotional trauma—the CDR can get “stuck” in the “on” position. This has devastating consequences for the ECM.
In a state of chronic CDR, cells like fibroblasts are signaled to go into overdrive. They begin to churn out excessive amounts of collagen, particularly the thick, rigid Type I collagen. They also produce enzymes that cross-link these fibers, making the ECM dense, stiff, and fibrotic. The once-fluid, gel-like matrix becomes more like hardened cement.
This densification and fibrosis of the fascia and ECM create a “cellular prison.”
Impaired Communication: The stiff matrix physically blocks the flow of signaling molecules, nutrients, and oxygen to the cells.
Waste Accumulation: Metabolic waste products cannot be efficiently cleared, creating a toxic local environment. This further lowers the local pH, making the tissue more acidic, which in itself is a powerful inflammatory signal.
Mechanical Entrapment: Nerves and blood vessels become compressed and entrapped within this fibrotic tissue, leading to pain, numbness, and ischemia (lack of blood flow).
Perpetuating Inflammation: The stiff ECM itself sends pro-inflammatory signals back to the cells, creating a vicious, self-perpetuating cycle of inflammation and fibrosis. This is a key driver of conditions like hyperalgesia (an amplified pain response) and sustained inflammation seen in chronic pain syndromes.
This process is not limited to musculoskeletal injuries. It is the same fundamental pathology we see in a fibrotic liver (cirrhosis), hardened arteries (atherosclerosis), and the tissue damage following chemotherapy or radiation. Understanding how to address and remodel this dysfunctional ECM is a cornerstone of true healing and longevity.
The Immune System’s Role in Fascia and the ECM
The immune system and the fascial/ECM network are inextricably linked. The ECM is not just a passive scaffold; it is a primary residence and playground for a vast array of immune cells. This is where the body’s surveillance and defense operations are headquartered.
Key immune cells that reside within the fascial matrix include:
Macrophages: the “clean-up crew” of the immune system. They patrol the ECM, engulfing cellular debris, pathogens, and senescent cells. They are also master regulators, capable of shifting their phenotype (behavior) from a pro-inflammatory (M1) state to an anti-inflammatory and pro-repair (M2) state. The state of the ECM heavily influences this shift.
Mast Cells: These cells are packed with granules containing potent signaling molecules like histamine and cytokines. When they degranulate in response to an injury or allergen, they initiate the inflammatory cascade, increasing blood vessel permeability and recruiting other immune cells to the site.
Lymphocytes (T cells and B cells): These are the cells of the adaptive immune system. They infiltrate tissues from the bloodstream in response to specific threats, orchestrating targeted attacks and creating immunological memory.
Dendritic Cells: These are the “scouts” that sample the environment for foreign invaders. They capture antigens and present them to T cells in lymph nodes, thereby initiating a specific immune response.
In a healthy state, these cells work in a beautifully orchestrated symphony. Following an acute injury, they mount a controlled inflammatory response to clear the damage and then transition to a pro-resolving phase to facilitate healing and remodeling of the ECM. This process is called immune tolerance and resolution.
Breaking the Tolerance: From Acute Inflammation to Chronic Disease
The problem arises when this process becomes dysregulated. In the context of a chronically stuck Cell Danger Response and a fibrotic ECM, the immune system’s behavior changes dramatically.
Vicious Cycle: The stiff, acidic, and hypoxic (low oxygen) ECM sends danger signals that keep macrophages in a pro-inflammatory M1 state. These M1 macrophages, in turn, release cytokines that stimulate fibroblasts to produce even more fibrotic tissue, perpetuating the cycle.
Loss of Tolerance: The normal resolution process fails. The immune system remains on high alert. T regulatory cells, which are supposed to pump the brakes on the immune response by releasing anti-inflammatory signals such as IL-10, become suppressed or ineffective.
Auto-reactivity: Chronic inflammation and tissue damage can expose “self-antigens”—proteins normally hidden from the immune system. This can trigger a case of mistaken identity, where the immune system begins to attack the body’s own tissues, leading to autoimmune diseases.
This breakdown of immune tolerance is a central driver of aging and chronic disease. It is the link between a local injury and systemic dysfunction. For example, a “leaky gut” (intestinal barrier hyperpermeability) allows bacterial components, such as lipopolysaccharide (LPS), to enter the bloodstream. This systemic inflammatory trigger can then break down the blood-brain barrier, allowing inflammation to spill into the central nervous system and activate microglia (the brain’s resident immune cells), contributing to neuroinflammation, brain fog, and chronic fatigue. The principles are universal: a breakdown in a barrier, a loss of immune tolerance, and a vicious cycle of inflammation.
The Case of the 19-Year-Old Woman: A Lesson in Immune Dysregulation
To make this tangible, let me share a clinical example. I recently worked with a 19-year-old young woman whose parents were concerned about her neurodivergent tendencies and a general lack of vitality. Her standard blood work was largely unremarkable, but a deeper dive revealed a story of profound immune dysregulation.
Her neutrophil count was persistently elevated. While neutrophils are our first responders to acute infection, chronically high levels suggest a state of sterile, low-grade inflammation. A closer look at her lymphocyte subsets and viral antibody panels told the real story. She had sky-high IgG antibodies to Epstein-Barr Virus (EBV).
Now, many people have been exposed to EBV. But her pattern was different. She had elevated antibodies to multiple viral components (VCA, EA, and EBNA), indicating a chronic, poorly controlled viral reactivation. Her immune system was “stuck” fighting a ghost. This constant battle was consuming vast amounts of energy and resources, contributing to her fatigue and neurological symptoms. Her immune system was unable to achieve resolution. It was locked in a state of perpetual, ineffective warfare, and her fascial and extracellular matrix environment was undoubtedly paying the price, becoming progressively more inflamed and dysregulated. This case highlights why we cannot look at any one system in isolation. Her neurological symptoms were a direct reflection of her immune dysregulation.
Metabolic Health: The Unseen Driver of Cellular Dysfunction
No discussion of cellular health and longevity is complete without a deep dive into metabolism, and specifically, the role of insulin. We live in an epidemic of metabolic dysfunction, and much of it is hidden, lurking beneath the surface of “normal” blood sugar readings.
The standard American diet, laden with processed carbohydrates and sugars, forces the pancreas to pump out large amounts of insulin to shuttle glucose out of the bloodstream and into cells. Over time, cells become resistant to this constant hormonal shouting. They “turn down the volume” on their insulin receptors. This is insulin resistance.
In response, the pancreas has to shout even louder, producing even more insulin to get the job done. This condition is called hyperinsulinemia (high insulin levels). For years, even decades, this compensatory mechanism can keep blood glucose levels in the “normal” range. The person’s A1C might be 5.5, and their fasting glucose might be 95 mg/dL. Their doctor tells them everything is fine.
But everything is not fine.
The Hidden Opportunity for Intervention
This period of “normoglycemic hyperinsulinemia” is a massive, missed opportunity for intervention. Insulin is a potent pro-growth and pro-inflammatory hormone. Chronically high levels of insulin are a powerful driver of the negative changes we’ve been discussing:
It promotes fat storage, particularly in the form of inflammatory white adipose tissue (WAT).
It directly stimulates inflammatory pathways.
It contributes to cell proliferation and can accelerate cancer growth.
It damages the endothelium (the lining of blood vessels), driving atherosclerosis.
It fuels the inflammatory processes within the ECM.
This is why it is absolutely critical to measure fasting insulin alongside fasting glucose and HbA1c. A fasting insulin level above 8 μIU/mL, and certainly above 10, is a major red flag, even if glucose is normal. I once had a physician patient whose fasting glucose was only 100 mg/dL, but his fasting insulin was over 30. He was on the brink of a metabolic catastrophe and didn’t even know it. This wasn’t a knowledge gap; it was a measurement gap. By addressing his profound hyperinsulinemia with targeted dietary changes, we averted a crisis.
The popular GLP-1 agonists work by improving insulin sensitivity and promoting satiety. While they can be powerful tools, they should never be used in a vacuum. If the underlying lifestyle and dietary habits that drive insulin resistance are not addressed, these drugs become a mere crutch. The foundation must be restoring the body’s natural insulin sensitivity through whole foods, proper nutrient timing, and movement. For example, simply adding glycine, an amino acid that can improve insulin signaling, can be a supportive measure alongside these broader strategies.
The Non-Surgical Approach to Wellness with Chiropractic Care- Video
Practical Interventions: Modulating the Fascial-Immune-Metabolic Axis
Understanding this complex interplay among the fascial system, the immune system, and our metabolism enables us to be much more strategic and precise in our interventions. The goal is to break the vicious cycles of inflammation and fibrosis and restore the body’s innate capacity for healing and resolution.
Heat and Cold: A Nuanced Approach
Thermotherapy (heat) and cryotherapy (cold) are ancient and powerful tools, but they are often used indiscriminately. Their effects are profoundly different, and their application must be timed correctly.
Cold Therapy (Cryotherapy): Cold causes vasoconstriction (narrowing of blood vessels) and has a potent acute anti-inflammatory effect. It slows down metabolic processes and reduces the initial swelling and pain signals immediately following an injury. Therefore, cold is best used for acute problems. Think of an athlete who just sprained their ankle. A short, targeted cold application can be very beneficial in the first 24-48 hours.
However, chronic, long-term use of cold can be counterproductive to healing. By persistently suppressing inflammation, you also suppress the signals necessary for repair and remodeling. You are essentially hitting the “pause” button on the healing process. Short-term application is key.
Heat Therapy (Thermotherapy): Heat causes vasodilation (widening of blood vessels), increasing blood flow to an area. This is crucial for the remodeling phase of healing. Increased blood flow brings in the oxygen and nutrients needed for fibroblasts to lay down new, healthy ECM. It also helps to flush out metabolic waste products that have accumulated in the area.
Therefore, heat is best used for chronic conditions, stiffness, and to promote the later stages of tissue repair after the acute inflammatory phase has subsided. It helps to make the fascial matrix more pliable and supports the long-term process of restoring tissue quality.
Clinical Guideline:
Acute Phase (0-72 hours post-injury): Use short-term, intermittent cold therapy to manage pain and swelling.
Subacute/Chronic Phase (After 72 hours): Transition to heat therapy to promote blood flow, tissue relaxation, and remodeling. Avoid daily, habitual cold plunging if your goal is tissue repair and adaptation.
Beyond Temperature: Photobiomodulation and Peptides
Modern science offers even more targeted ways to influence this system.
Photobiomodulation (PBM) / Red Light Therapy: This involves exposing the body to specific wavelengths of red and near-infrared light. The mitochondria, the powerhouses of our cells, absorb this light energy. The primary effect is to stimulate ATP production (cellular energy) and, in a controlled manner, transiently increase reactive oxygen species (ROS), triggering the body’s antioxidant and repair mechanisms. PBM can reduce inflammation, stimulate fibroblast activity for healthy collagen production, improve circulation, and modulate the immune response. It is a powerful tool for changing the phenotypic expression of cells—shifting them from a “danger” state to a “healing” state.
Peptides: Peptides are short chains of amino acids that act as precise signaling molecules. They offer a way to give the body specific instructions. For example, BPC-157 (Body Protection Compound-157) is a peptide that has been shown in extensive research to accelerate the healing of a wide variety of tissues—muscle, tendon, ligaments, and even the gut lining. It appears to work by promoting angiogenesis (the formation of new blood vessels), modulating growth factor signaling, and protecting the endothelial barrier. When dealing with a “leaky gut” or a chronic tendon injury, BPC-157 can be a remarkable tool for restoring barrier integrity and facilitating repair.
The ultimate strategy involves a multi-pronged approach. We must change the terrain. This means cleaning up the diet to reverse hyperinsulinemia, using strategic movement to hydrate and mobilize the fascia, managing stress to calm the nervous system, and then layering in targeted therapies like PBM or peptides to provide the specific signals the body needs to break out of chronic dysfunction and re-engage its powerful, innate healing programs.
Disclaimer
The information contained in this educational post is for informational purposes only and is not intended to be a substitute for professional medical advice, diagnosis, or treatment. It is not intended for self-diagnosis or to replace a qualified healthcare professional’s consultation. Dr. Alex Jimenez, DC, FNP-APRN, is not your medical provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this web page. All individuals must obtain recommendations for their personal situations from their own medical providers. Reliance on any information provided in this post is solely at your own risk.
Summary, Conclusion, and Key Insights
Summary
This educational post has provided a comprehensive overview of a modern, systems-based approach to health, longevity, and the treatment of chronic conditions. We began by redefining aging as a modifiable biological process, emphasizing the critical need for establishing a physiological baseline early in life for predictive and personalized medicine. We then delved into the profound importance of the fascial system and the Extracellular Matrix (ECM), recasting them as a dynamic, body-wide sensory and communication network rather than passive structural elements. We explored how this network’s health is determined by the behavior of cells such as fibroblasts, and how chronic inflammation and the Cell Danger Response (CDR) can lead to fibrosis, creating a “cellular prison” that impairs function and perpetuates disease. The intimate relationship between the fascial/ECM environment and the immune system was highlighted, explaining how immune dysregulation and a loss of tolerance can drive chronic inflammatory and autoimmune conditions. Furthermore, we identified hyperinsulinemia as a key, often hidden, metabolic driver of this systemic inflammation. Finally, we translated this complex physiology into a practical intervention framework, discussing the nuanced application of heat and cold therapies and introducing advanced modalities such as photobiomodulation and peptides as targeted tools to restore cellular function, modulate the immune response, and promote tissue remodeling.
Conclusion
The future of medicine lies in moving beyond siloed symptom-based treatment and embracing a holistic understanding of the body’s interconnected systems. The fascial network, the immune system, and our metabolic state are not separate entities; they are in constant, dynamic conversation. Health and vitality are emergent properties of a well-functioning, resilient biological system, while chronic disease results from a system stuck in a vicious cycle of dysfunction. By understanding the underlying physiology—from the densification of the ECM to the subtleties of immune cell signaling and the devastating impact of metabolic dysregulation—we can shift our focus from merely managing disease to actively cultivating health. The ultimate therapeutic strategy addresses the root causes: it cleans up the cellular environment, restores proper signaling, provides the necessary resources for repair, and empowers the body’s innate intelligence to heal itself. This evidence-based, integrative approach is the most powerful and promising path toward extending not just our lifespan, but our healthspan.
Key Insights
Aging is Modifiable: View aging not as a fixed timeline but as a collection of biological processes (the “Hallmarks of Aging”) that can be influenced by lifestyle, environment, and targeted interventions.
The Baseline is Everything: Proactively establishing a comprehensive biological baseline is the cornerstone of preventive and personalized medicine, enabling early detection of physiological deviations.
Fascia is an Intelligent System: Your fascial network is a primary sensory and communication organ, not just structural “stuff.” Its health is paramount for overall well-being, movement, and cellular communication.
The ECM Dictates Cellular Health: The state of the Extracellular Matrix—whether it is hydrated and fluid or dense and fibrotic—directly controls the function, survival, and behavior of every cell in your body.
The Cell Danger Response (CDR) is a Vicious Cycle: A chronically activated CDR leads to a self-perpetuating cycle of inflammation and fibrosis, which is a root cause of many chronic pain and disease states.
Measure Fasting Insulin: “Normal” blood sugar can mask dangerous hyperinsulinemia, a potent driver of chronic inflammation and metabolic disease. Measuring fasting insulin is a critical, non-negotiable health metric.
Interventions Must Be Strategic: Therapies like heat, cold, PBM, and peptides are powerful but must be applied with a nuanced understanding of their physiological effects and the specific stage of tissue healing to be effective. The goal is to break the cycle of dysfunction and restore the body’s innate healing capacity.
López-Otín, C., Blasco, M. A., Partridge, L., Serrano, M., & Kroemer, G. (2013). The hallmarks of aging. Cell, 153(6), 1194-1217.
Schleip, R., Jäger, H., & Klingler, W. (2012). What is fascia? A review of different nomenclatures. Journal of Bodywork and Movement Therapies, 16(4), 496-502.
Naviaux, R. K. (2014). Metabolic features of the cell danger response. Mitochondrion, 16, 7-17.
Myers, T. W. (2014). Anatomy Trains: Myofascial Meridians for Manual and Movement Therapists. 3rd ed. Churchill Livingstone.
Franceschi, C., & Campisi, J. (2014). Chronic inflammation (inflammaging) and its potential contribution to age-associated diseases. The Journal of Gerontology: Series A, 69(Suppl_1), S4-S9.
Crofts, C. A., Zinn, C., & Wheldon, M. (2015). The case for a low-carbohydrate diet in the management of type 2 diabetes. Expert Review of Clinical Pharmacology, 8(3), 263-265. [Note: Thematic reference for hyperinsulinemia concept].
Hamblin, M. R. (2017). Mechanisms and applications of the anti-inflammatory effects of photobiomodulation. AIMS Biophysics, 4(3), 337-361.
Seiwerth, S., Sikiric, P., et al. (2018). BPC 157 and standard angiogenic growth factors. Synergistic effects of BPC 157 and VEGF. Current Pharmaceutical Design, 24(18), 1972-1989.
Bordoni, B., & Mahabadi, N. (2021). Fascia, Function, and Medical Applications. In StatPearls. StatPearls Publishing.
Langevin, H. M., & Sherman, K. J. (2007). Pathophysiological model for chronic low back pain integrating connective tissue and nervous system mechanisms. Medical Hypotheses, 68(1), 74-80.
Have you ever felt awful after eating too much candy or sugary snacks? You might wonder if it’s possible to experience a sugar hangover. Certainly, a “sugar hangover” is a genuine, transient phenomenon that is marked by irritability, fatigue, headache, and brain fog. It is a consequence of a sudden increase in blood sugar levels, followed by an abrupt decline. Dehydration and hormonal fluctuations are frequently the result of consuming excessive amounts of sugar or refined carbohydrates.
This feeling is not just in your head. Many people report it after holidays or parties with lots of sweets. In this article, we’ll explain what a sugar hangover is, why it happens, and how to feel better. We’ll also look at long-term risks and ways professionals like chiropractors and nurse practitioners can help.
What Is a Sugar Hangover?
A sugar hangover happens when you eat a lot of sugar or simple carbs, like white bread or candy. Your body converts these into glucose quickly, which then enters your blood. This can raise your blood sugar quickly. Then, your body tries to fix it by releasing insulin from the pancreas. Insulin helps move the glucose into cells for energy or storage. But sometimes, this causes blood sugar to drop too low too soon. That’s called reactive hypoglycemia.
This up-and-down cycle can make you feel sick for a few hours. It’s different from an alcohol hangover, but sugar can make alcohol hangovers worse by hiding the taste of booze, leading to more drinking. Sugar hangovers are real and backed by science. They mess with your hormones and energy levels.
For people with diabetes, it’s even more serious. High blood sugar in the morning can cause fogginess, irritability, and other symptoms. This is due to factors like the Dawn phenomenon, in which hormones prompt the liver to release extra glucose early in the day.
Common Symptoms of a Sugar Hangover
Symptoms can start soon after eating sweets and last a few hours. They come from high blood sugar (hyperglycemia) and then low blood sugar (hypoglycemia). Here’s a list of common ones:
Fatigue and low energy, like you need a nap.
Headache or migraine-like pain.
Brain fog makes it challenging to think clearly.
Irritability or mood swings.
Shakiness, sweating, or anxiety from the sugar crash.
Increased thirst and dehydration.
Blurred vision or dizziness.
Hunger or cravings for more sugar.
Nausea or stomach upset.
These feel like a mild flu or a bad day. If severe, such as very low blood sugar, it can be dangerous, but that’s rare in healthy people.
Causes Behind Sugar Hangovers
The main cause is eating too much added sugar or refined carbs without other foods to slow it down. Simple sugars digest fast, spiking blood sugar. Your body overreacts with too much insulin, causing a crash.
Other factors include:
Eating sweets on an empty stomach.
Mixing sugar with alcohol.
Dehydration occurs when sugar pulls water into your blood.
Hormone changes, such as increased cortisol or adrenaline.
Poor sleep or stress makes your body less able to handle sugar.
Sugar affects your brain, too. It gives a quick high but then leaves you foggy because glucose is the brain’s main fuel. When levels swing, your thinking suffers.
In diabetes, mistakes like not checking blood sugar at night or wrong insulin use can lead to morning hangovers.
Long-Term Health Risks of Frequent Sugar Hangovers
Although the immediate symptoms are transient, the long-term health consequences of frequent, high-sugar consumption may occur. Over time, repeated spikes can lead to insulin resistance. This means your body doesn’t respond well to insulin, raising risks for type 2 diabetes.
Other risks include:
Damage to blood vessels, leading to heart disease or stroke.
Weight gain from extra calories.
Inflammation in the body.
Higher chance of kidney or eye problems.
Addiction-like cravings for sugar.
The World Health Organization recommends keeping sugar to less than 10% of your daily calories. For 2,000 calories, that’s about 50 grams or less. Eating lots often can harm your health slowly.
How to Recover from a Sugar Hangover
Feeling bad? You can recover with simple steps. Focus on balancing your body.
Here are key recovery tips:
Drink plenty of water to flush out sugar and rehydrate. Add lemon for flavor.
Eat balanced meals with protein, healthy fats, and fiber, like eggs with veggies or nuts.
Get light exercise, like a walk, to boost circulation and endorphins.
Rest well so your body can heal.
Have nutrient-rich foods, such as greens, fruits, or yogurt, for gut health.
Avoid more sugar or alcohol.
For quick relief, try a protein smoothie or a green juice. If you have diabetes, check your blood sugar and talk to a doctor.
Preventing Sugar Hangovers in the Future
Prevention is better than recovery. Make smart choices to avoid spikes.
Tips include:
Pair sweets with protein or fat to slow absorption.
Choose complex carbs like whole grains or veggies.
Use the glycemic index to pick low-spike foods.
Limit added sugars daily.
Stay hydrated and active.
Eat regular meals to keep blood sugar steady.
Walk after meals to use up glucose. For holidays, plan balanced snacks.
Integrative Care for Sugar Hangovers and Blood Sugar Issues
“Sugar hangovers”—the fatigue, inflammation, and migraines that result from excessive sugar consumption—are addressed by integrative chiropractic care and nurse practitioners (NPs) through the holistic treatment of the body. NPs offer metabolic, dietary, and lifestyle support to reduce inflammation and promote detoxification, while chiropractors optimize nervous system function to support blood sugar regulation.
A potent, multifaceted approach that addresses both the structural and chemical imbalances resulting from excessive sugar consumption is provided by the combination of chiropractors and nurse practitioners.
Chiropractors fix spine misalignments to improve nerve flow. This helps the body better regulate insulin and glucose. Studies show it can lower blood sugar markers, such as hemoglobin A1C, and reduce pain from diabetes.
Benefits of chiropractic for blood sugar:
Better nerve function for insulin control.
Less stress and inflammation.
Improved circulation and healing.
Lifestyle advice on diet and exercise.
NPs help with diet plans, supplements like magnesium or fish oil, and detox habits. They monitor health and work with chiropractors for comprehensive care.
This holistic approach looks at the “3 Ts”: thoughts (stress), trauma (injuries), and toxins (such as sugar). Reducing these helps prevent issues.
Clinical Observations from Dr. Alexander Jimenez
Dr. Alexander Jimenez, DC, APRN, FNP-BC, a chiropractor and nurse practitioner in El Paso, Texas, shares insights from over 30 years of practice. He uses integrative care for blood sugar issues, focusing on root causes such as inflammation and gut health. In his work, he sees sugar overconsumption leading to fatigue and pain, similar to hangovers. He combines adjustments, nutrition, and detox plans to help patients recover and manage diabetes without drugs when possible.
Dr. Jimenez notes that spinal adjustments improve nerve signals to the pancreas, thereby aiding insulin secretion. He recommends supplements for blood sugar and stresses the importance of exercise to fight metabolic issues. His clinic helps with neuropathy and injuries tied to poor sugar control.
Conclusion
Yes, sugar hangovers are real and can make you feel terrible from blood sugar swings. By understanding causes and using recovery tips, you can feel better fast. For ongoing issues, consider integrative care from chiropractors and NPs. Eat smart, stay active, and listen to your body to avoid them.
Many people expect sciatica to feel like low back pain that shoots down the leg. But a very common (and confusing) version is this:
Your lower back feels okay
Your hamstring, calf, foot, or toes feel numb, tingly, or “asleep”
That can still be sciatica—or a condition that mimics sciatica. The key is understanding that sciatica is a symptom pattern, not a single diagnosis. It occurs when nerve tissue supplying the sciatic nerve pathway becomes irritated, compressed, or sensitized. (Penn Medicine, n.d.; Yale Medicine, n.d.; HSS, 2024)
At ChiroMed (chiromed.com), a practical way to approach this is to ask two questions:
Where is the nerve getting irritated? (low back vs. buttock/hip vs. near the hamstring)
What’s keeping it irritated? (movement habits, muscle tension, joint mechanics, posture, and load)
This article explains why leg numbness can happen without back pain, how to tell it apart from a hamstring strain, when to seek care, and how an integrative chiropractic plan can support recovery—while coordinating with medical evaluation when needed.
What “Sciatica” Really Means (Simple Definition)
Sciatica describes symptoms that follow a nerve pathway—usually from the buttock down the back or side of the leg. Symptoms may include:
Numbness
Tingling (“pins and needles”)
Burning or “electric” sensations
Sharp or aching pain
Weakness in the leg or foot (in more serious cases) (HSS, 2024; Yale Medicine, n.d.; Penn Medicine, n.d.)
Important point: You can have numbness and tingling with minimal pain, and you can have leg symptoms even when your low back does not hurt. (Penn Medicine, n.d.; Yale Medicine, n.d.)
Why Your Hamstring and Foot Can Go Numb Without Back Pain
People often say, “If my back doesn’t hurt, how could this be sciatica?” Here are common explanations.
The “problem spot” and the “felt spot” can be different
Nerves are like wiring. If a nerve is irritated higher up, you may feel symptoms farther down. That’s why a nerve issue can feel like a hamstring or foot problem. (Penn Medicine, n.d.; HSS, 2024)
The irritation may be in the hip or buttock region
Sometimes the sciatic nerve is irritated by muscles and connective tissue in the buttock area. A well-known example is piriformis syndrome, where deep hip muscles contribute to sciatic-type symptoms. People may feel:
Buttock tightness
Hamstring “numb soreness”
Tingling in the calf or foot
Symptoms worsen with sitting or driving (Total Ortho Sports Med, 2025)
Clinical observation used in integrative care: when the pelvis and hip are not moving well, deep hip muscles may tighten as “helpers,” which can increase nerve irritation in certain people—especially if they sit a lot, train hard, or have uneven movement patterns. (Jimenez, n.d.-a)
A spinal cause can still exist even if your back feels fine
Even without back pain, symptoms can still come from the lumbar spine, such as:
Disc irritation (bulge/herniation)
Narrowing around nerve roots (stenosis)
Other mechanical or inflammatory causes (HSS, 2024; Penn Medicine, n.d.)
This is one reason careful evaluation matters: no back pain automatically rules out the spine.
The nerve may be irritated closer to the hamstring
Some people get sciatic nerve irritation near where the hamstring attaches to the high part of the pelvis. This can feel like:
Deep buttock pain
“Hamstring tightness” that won’t stretch out
Tingling or numbness down the leg (Jimenez, 2025)
Sciatica vs. Hamstring Strain: How to Tell the Difference
This is one of the most common questions ChiroMed patients ask, because the symptoms can overlap.
Hamstring strain tends to look like this
A clear injury moment (sprint, slip, kick, deadlift)
Local pain in the back of the thigh
Pain when you stretch the hamstring
Pain when you contract the hamstring
Tenderness or bruising (in some cases) (Ducker Physio, 2025)
Sciatica-type nerve symptoms tend to look like this
Tingling, buzzing, burning, or numbness
Symptoms that travel below the knee (often into the foot)
Symptoms that change with posture (sitting, bending, driving)
Sensations that feel “electric” or “deep” rather than sore-muscle pain (HSS, 2024; Ducker Physio, 2025)
Quick comparison:
More muscle: sharp pull + local tenderness + pain with stretch
More nerve: numbness/tingling + travel to foot + posture-dependent changes
If you are unsure, it’s safer to get assessed—because the best treatment plan depends on the true cause.
Why Numbness Deserves Respect (Even If Pain Is Mild)
Pain is loud. Numbness can be quiet, but it can signal that a nerve is not communicating well.
The American Medical Association notes that leg numbness or weakness can be an atypical symptom that warrants evaluation—especially if it progresses or is accompanied by other warning signs. (AMA, 2024)
At ChiroMed, a “rule of thumb” approach is:
Occasional tingling that improves quickly may respond well to conservative care.
Persistent or worsening numbness, especially with weakness, should be evaluated more urgently.
Red Flags: When You Should Seek Care Quickly
Seek urgent medical evaluation if you have:
New or worsening leg weakness
Foot drop (difficulty lifting the front of the foot)
Loss of bowel or bladder control
Numbness in the “saddle” area (inner thighs/groin)
Severe symptoms that rapidly worsen (AMA, 2024; Penn Medicine, n.d.)
Also, schedule an evaluation soon if:
Numbness lasts longer than 1–2 weeks
Symptoms keep returning
Symptoms spread farther down the leg
You can’t work, train, or sleep normally (Penn Medicine, n.d.; HSS, 2024)
What a Good Evaluation Usually Includes
A careful sciatica-style workup often checks:
Where symptoms travel (hamstring only vs. foot/toes)
What triggers symptoms (sitting, bending, walking, lifting)
Sensation, strength, and reflexes
Hip and pelvic motion
Nerve tension testing
Whether imaging is needed (HSS, 2024; Penn Medicine, n.d.)
Why this matters: many conditions can look like sciatica. There are “musculoskeletal mimics” that can imitate nerve-root problems, so testing needs to be specific and organized.
ChiroMed’s Integrative Approach: What It Tries to Fix (Not Just “Chase Pain”)
When sciatica shows up mainly as hamstring and foot numbness, an integrative chiropractic plan often focuses on:
1: Reduce nerve irritation
Goal: decrease mechanical and inflammatory stress on the nerve pathway.
Goal: improve how the low back, pelvis, and hip share load.
This may include:
Lumbar and pelvic mobility work (as appropriate)
SI/hip mechanics support
Posture strategies for sitting/driving (especially for desk workers) (Total Ortho Sports Med, 2025)
Clinical observations commonly emphasized in integrative settings: many recurring sciatica patterns involve combined issues—restricted hip motion, overworked deep hip muscles, and poor load sharing through the pelvis and lumbar spine—especially in active adults and people who sit long hours. (Jimenez, n.d.-a)
3: Build strength and control so symptoms don’t keep returning
Goal: stop the “flare-up cycle.”
Common focus areas:
Glute strength/endurance (hip stability)
Core/trunk control
Gradual return to lifting or sport
Movement retraining (how you hinge, squat, run, or climb) (HSS, 2024)
Common Tools Used in Integrative Chiropractic Care
Different people need different tools. The main idea is to match the tool to the driver.
Spinal and pelvic adjustments (when appropriate)
These are used to support joint motion and reduce mechanical stress in a region that may be contributing to nerve irritation. They are often paired with exercise and education rather than used alone. (Auburn Hills Chiropractic, n.d.)
Soft-tissue therapies
These may target:
Piriformis and deep hip rotators
Glutes
Hamstrings (especially the upper attachment area)
Surrounding fascia and trigger points (Total Ortho Sports Med, 2025)
Corrective exercises (the “long-game”)
These often include:
Hip mobility drills
Glute activation work
Controlled hamstring loading (when appropriate)
Core stability patterns
Walking progression and graded exposure back to activity (HSS, 2024)
Co-management with medical evaluation when needed
Many sciatica cases respond to conservative care, but persistent numbness, weakness, or red flags may require imaging and medical management. (Penn Medicine, n.d.; AMA, 2024)
Clinical practice guidelines often support care that includes:
Education
Exercise-based rehab
Manual therapy as part of a broader plan (Zaina et al., 2023)
At-Home Habits That Often Help (Simple, Practical)
These are not a diagnosis, but they can reduce flare-ups while you get evaluated.
Helpful habits
Take short walking breaks if sitting triggers symptoms
Avoid staying in one position too long
Use a pillow or support to reduce slumped sitting
Reduce aggressive stretching if it increases tingling
Keep training “in the safe zone” (no sharp increases in symptoms) (HSS, 2024)
Things that often make it worse
Long car rides without breaks
Deep forward bending early on (for some people)
“Stretching harder” into nerve symptoms
Ignoring weakness or worsening numbness (AMA, 2024; Penn Medicine, n.d.)
What Recovery Usually Looks Like
Many people improve over weeks to a few months with conservative care and good movement habits.
Step 3: return to normal activity with fewer flare-ups
The biggest mistake is trying to “rush” flexibility or intensity while the nerve is still irritated. For nerve symptoms, calm, consistent progress usually beats aggressive pushing.
Key Takeaways (Fast Summary)
Sciatica can cause hamstring and foot numbness without low back pain. (Penn Medicine, n.d.; Yale Medicine, n.d.; Total Ortho Sports Med, 2025)
Causes can include hip/buttock-region irritation (piriformis-related), lumbar nerve root irritation, or local nerve irritation near the hamstring. (HSS, 2024; Jimenez, 2025)
Numbness and weakness matter, especially if worsening or paired with red flags. (AMA, 2024)
An integrative plan—like the approach used at ChiroMed—often combines manual care, soft-tissue work, and corrective exercise to restore movement, reduce nerve stress, and prevent repeat flare-ups. (Zaina et al., 2023)
Zaina, F., et al. (2023). A systematic review of clinical practice guidelines for low back pain with and without radiculopathy. Archives of Physical Medicine and Rehabilitation. https://pubmed.ncbi.nlm.nih.gov/36963709/
Enhance your vitality with Neuro-Metabolic Strategies designed to support overall wellness and performance.
Abstract (Introduction
As a clinician bridging chiropractic neuro-functional care with advanced family practice nursing, I’ve witnessed a striking convergence of metabolic physiology, neurochemistry, and behavioral medicine. In this educational post, I present an integrated, evidence-based exploration of how neuroendocrine signaling—particularly involving the striatum, dopamine, serotonin, and inflammatory mediators—shapes obesity risk, mood regulation, impulse control, and human performance. Drawing on modern methodologies including neuroimaging, metabolomics, randomized clinical trials, and real-world implementation science, I translate key findings from leading researchers into practical, patient-centered approaches.
We will explore how alterations in the striatal dopamine system—especially reductions in dopamine D2 receptor density—are linked with obesity, compulsive food seeking, and reward dysregulation, and how targeted interventions—nutrition, movement, sleep, stress modulation, and precision supplementation—can recalibrate these systems. We will examine the serotonergic system,focusing on tryptophan metabolism, indoleamine 2,3-dioxygenase (IDO), and the kynurenine pathways, detailing how inflammation diverts tryptophan away from serotonin production, potentially worsening mood symptoms and fatigue, while creating opportunities for dietary, lifestyle, and clinical strategies to restore balance.
We will assess cardiovascular autonomic regulation—blood pressure variability, sympathovagal balance, and endothelial function—showing how structural and functional integrity in the vascular and neural systems can be influenced through exercise prescriptions, breathing techniques, sleep hygiene, and nutraceuticals like omega-3s, magnesium, and polyphenols. We will discuss the role of gut-derived signals, microbiome-related metabolites, and neuromodulatory oils in modulating neurotransmitter balance and systemic inflammation.
The post also integrates structured habit architecture—my “ABCs of self-led program design”—to help patients build sustainable routines. This framework leverages principles from motivational interviewing, cognitive-behavioral strategies, and reinforcement learning, empowering individuals to translate biochemical insights into daily practice. We will consider how culture and community shape metabolic choices, and how clinicians can provide practical, realistic recommendations grounded in implementation science to reduce “knowing-doing gaps.”
Throughout, I present clinical vignettes and relatable examples, explaining why each technique is used, what physiology it targets, and how to personalize protocols based on biomarker patterns, symptoms, and patient preferences. We will cover common misconceptions—like “zero-carb alcohol is harmless”—and clarify how the brain’s reward circuitry oversimplifies such claims, often undermining long-term goals.
Finally, we synthesize these themes into a practical map: how to read metabolic and neurochemical signals; how to select interventions that support resilience in the brain, gut, and vascular systems; and how to coach behavior change so improvements endure. The goal is to provide a comprehensive, readable, clinically grounded resource—modern, integrative, and compassionate—for patients, caregivers, and fellow clinicians who want to harness the power of neuroendocrine health to improve weight, mood, energy, and performance.
Neuroendocrine Foundations: Metabolic Health and Reward Circuitry in Obesity
In clinical practice, I frequently encounter patients whose metabolic challenges—weight gain, food cravings, mood variability—are not simply “lack of willpower” but reflections of disrupted neurobiological signaling. A critical hub is the striatal complex, part of the basal ganglia, which integrates dopaminergic input from the ventral tegmental area and substantia nigra, modulating motivation, reward valuation, habit formation, and movement.
Dopamine D2 Receptors, Obesity, and Compulsive Eating
Several landmark studies demonstrate that individuals with obesity often exhibit reduced striatal D2 receptor availability. Positron emission tomography (PET) imaging with radioligands like [11C]raclopride has shown that this reduction correlates with diminished sensitivity to natural rewards. The brain adapts to constant hyperpalatable stimulation—high levels of sugar, fat, and salt—by downregulating receptors. As D2 receptor density decreases, the brain requires more intense stimulation to reach the same level of reward. Clinically, this presents as:
Heightened cravings and difficulty feeling satisfied with normal portions
Compulsive eating behaviors driven by reward-seeking rather than hunger
Decreased motivation for non-food rewards (exercise, social engagement) due to reward dampening
Why use targeted interventions? Because dopamine signaling is plastic. Positive behavior changes—such as exercise, adequate protein intake, and circadian-aligned sleep—can upregulate receptor expression and improve reward responsivity.
Physiology: Striatum and Behavior
The striatal direct and indirect pathways coordinate movement and reinforcement learning. D1 receptor activation supports direct pathway facilitation, while D2 receptor activation inhibits the indirect pathway, promoting smoother action selection. Nutritional excess, sleep loss, and chronic stress alter dopamine synthesis and receptor turnover, shaping habit loops. Over time, the interplay between dopaminergic tone and inflammatory signaling further erodes reward control.
Clinical Strategy: Restoring Reward Balance
I use a staged plan:
Stabilize glycemic variability to avoid dopamine volatility
Rebuild sleep architecture and circadian rhythm to support dopamine synthesis
Implement structured exercise to enhance receptor sensitivity
Deploy protein-first eating to maintain satiety and reduce hyperpalatable triggers
Introduce micro-goals: small changes that recondition the reward system
Patients often report that cravings decline before weight changes appear, a sign that neural recalibration is starting.
Serotonin, Tryptophan, and the IDO–Kynurenine Axis: Mood, Inflammation, and Energy
Serotonin Biology: Beyond “Feel-Good”
Serotonin (5-HT) is synthesized from the essential amino acid tryptophan, primarily via the enzyme tryptophan hydroxylase. In the CNS, serotonin regulates mood, impulse control, sleep, and appetite. In the gut, it influences motility and interacts with microbial signals.
However, under inflammatory stress, tryptophan metabolism can shift dramatically. The enzyme indoleamine 2,3-dioxygenase (IDO), activated by inflammatory cytokines like IFN-γ, TNF-α, and IL-6, diverts tryptophan away from serotonin synthesis into the kynurenine pathway. Downstream metabolites—kynurenine, 3-hydroxykynurenine, quinolinic acid—can be neuroactive and neurotoxic in excess, affecting glutamatergic signaling and oxidative stress.
Why the IDO Pathway Matters Clinically
When IDO activity is elevated, patients may experience:
This can coexist with obesity, insulin resistance, and cardiovascular risk. The physiology links systemic inflammation with serotonergic depletion and glutamatergic over-excitation. When patients tell me, “I feel off,” I often consider the tryptophan-to-kynurenine ratio as part of the workup.
Support micronutrients: vitamin B6, B2, folate, B12, magnesium, and iron optimize monoamine synthesis
Promote exercise: skeletal muscle expresses kynurenine aminotransferases (KATs) that convert potentially neurotoxic kynurenine to kynurenic acid, which is less likely to cross the blood-brain barrier—exercise therefore serves as a “peripheral sink.”
Encourage polyphenol-rich foods, such as berries, green tea, olive oil, and crucifers, as they attenuate NF-κB activation and may downregulate IDO.
Optimize gut function: microbial composition influences tryptophan availability and ENS serotonin signaling.
The rationale: modulating inflammation and supporting micronutrients recalibrates tryptophan allocation, enhancing serotonin availability and reducing the neurotoxic burden of quinolinic acid.
Exploring Integrative Medicine- Video
The ABCs of Self-Led Program Design: A Practical Framework
I often teach patients a simple, powerful habit architecture—my ABCs—to make physiological gains sustainable.
A: Anchor – Tie a desired action to a reliable cue. Example: “After brushing teeth, I will prepare my protein-forward breakfast.” Anchors leverage existing routines to reduce decision fatigue.
B: Build – Start small and build complexity gradually. Example: begin with 10 minutes of brisk walking, expand to interval training as fitness improves. Building protects dopamine balance by avoiding overwhelm.
C: Consistency – Aim for daily consistency rather than intensity. Consistency creates predictable dopamine reinforcement, embedding habits into basal ganglia pathways.
Why this works: It aligns the brain’s habit circuitry—dorsal striatum—and reward prediction error mechanisms. Each completed action delivers a small dopamine signal, strengthening the routine. The ABCs reduce cognitive load, which is crucial when stress or inflammation impairs executive function.
Cardiovascular Autonomics and Blood Pressure: Sympathovagal Balance
Patients often ask, “How do I lower my blood pressure naturally?” Autonomic tone—balance between sympathetic and parasympathetic activity—plays a central role.
Physiology Essentials
Sympathetic activation increases heart rate, vasoconstriction, and renin release.
Endothelial health governs vascular reactivity and inflammation
Evidence-Based Interventions and Rationale
Breathing training: slow diaphragmatic breathing (5–6 breaths/min) enhances vagal tone, reduces sympathetic outflow, and improves baroreflex. Patients often experience immediate calm and modest reductions in BP.
Aerobic and resistance exercise improve endothelial NO availability, reduce arterial stiffness, and lower resting sympathetic activity.
Sleep optimization: treating sleep apnea reduces catecholamines and blood pressure.
Dietary strategies: DASH-style patterns, potassium-rich foods, magnesium intake, and nitrates (beetroot) support vasodilation and pressure control.
Nutraceuticals: omega-3 fatty acids reduce inflammation and improve endothelial function; magnesium supports vascular tone; polyphenols modulate oxidative pathways in the endothelium.
The aim: strengthen vascular resilience and autonomic balance rather than relying solely on acute fixes.
Gut–Brain Axis: Microbiome, Oils, and Neurotransmitter Modulation
The gut microbiome shapes neurochemical balance via short-chain fatty acids (SCFAs), tryptophan metabolites, and immune signaling. Patients sometimes mention “gland-regulating oils”—in my practice, I interpret this as adaptogenic or neuromodulatory oils (e.g., omega-3s, evening primrose, black seed oil) that may support endocrine and inflammatory balance. While terminology varies, the principle is consistent: lipids profoundly affect cell membranes, receptor function, and signaling.
Physiological Rationale
Omega-3s are incorporated into neuronal membranes, improving membrane fluidity and signaling in dopaminergic and serotonergic synapses.
SCFAs (butyrate) strengthen gut barrier integrity, reducing LPS translocation and systemic inflammation that drives IDO.
Polyphenols and specific oils modulate NF-κB and JAK/STAT pathways, dampening inflammatory cascades.
Clinical Application
I recommend a food-first approach (fatty fish, olives, nuts, seeds) complemented by targeted supplementation when needed. Patients with mood and metabolic disturbances often benefit from EPA-dominant omega-3s, and those with inflammatory skin or PMS may respond to GLA-containing oils.
Clarifying Misconceptions: “Zero-Carb Alcohol” and Reward Systems
A common assertion is “tequila has zero carbs; it’s fine.” While certain spirits may have minimal carbohydrates, they are not metabolically neutral.
Why Alcohol Complicates Metabolic and Neurochemical Goals
Hepatic ethanol metabolism disrupts the NAD+/NADH balance, impairing fatty acid oxidation and promoting hepatic steatosis in excess.
Alcohol modulates GABA and glutamate, interacts with dopamine pathways, and can enhance reward-seeking behaviors.
Sleep disruption: alcohol fragments sleep, reduces REM, and worsens next-day cravings and mood
Appetite and judgment: alcohol lowers inhibitory control, increasing the likelihood of high-calorie intake
Clinical advice: If patients choose to drink, set clear boundaries, pair with protein, hydrate, and prioritize sleep. Recognize the reward circuitry effects—alcohol may rekindle old habits.
Practical Tools: Data-Guided Personalization
Patients often ask: “What data should I track?” I suggest:
Weight and waist circumference: visceral adiposity correlates with inflammation and cardiometabolic risk
Blood pressure, heart rate variability (HRV): markers of autonomic balance
Sleep metrics: duration, consistency, apnea risk
Mood and energy logs: identify patterns with nutrition, alcohol, and stress
Food journal: highlight triggers, portions, protein intake
Why data matter: They transform subjective experiences into observable trends, allowing tailored interventions—e.g., adjusting protein timing when afternoon cravings surge, or adding evening breathing exercises when HRV dips.
Protein-First Strategy and Satiety Physiology
Protein influences satiety through peptide YY, GLP-1, and cholecystokinin signaling. Adequate protein supports dopamine synthesis by increasing tyrosine availability and stabilizes glucose levels, reducing reward volatility.
Practical approach:
Aim for 1.2–1.6 g/kg/day, adjusted for renal function and activity
Distribute protein across meals to sustain satiety
Pair with fiber-rich vegetables to slow gastric emptying and blunt glycemic excursions
Rationale: Stabilized satiety reduces hedonic eating, enabling the brain to recalibrate D2 receptor signaling.
Sleep Architecture: Dopamine and Serotonin Restoration
Poor sleep reduces dopamine tone and impairs prefrontal control, worsening impulsivity. Serotonin contributes to sleep onset and stability.
Interventions:
Fixed sleep-wake times to stabilize circadian rhythm
Dim evening light; increase morning light exposure
Limit alcohol and heavy meals near bedtime
Consider magnesium glycinate, behavioral strategies, and screening for sleep apnea.
Clinical correlation: Improved sleep often leads to fewer cravings, better mood, and enhanced exercise adherence.
Exercise Prescriptions: Receptor Plasticity and Kynurenine Metabolism
Regular exercise increases D2 receptor availability, improves insulin sensitivity, and shifts kynurenine toward kynurenic acid via muscle KAT activity.
Programming:
Begin with a manageable aerobic base (e.g., brisk walking 20–30 minutes)
Add resistance training to improve myokine signaling and metabolic reserves
Progress to intervals or sport-based activity to maintain engagement
Why it works: Exercise is a systemic signal—improves vascular health, neuroplasticity, and mood—creating compounding benefits.
Stress Modulation: Cortisol, Catecholamines, and Reward Control
Plan social settings: eat before events, pre-commit to limits
Why: Reduces choice overload and reward temptation, enabling dopamine recalibration to proceed uninterrupted.
Clinical Vignettes: Real-Life Applications
Patient A: Middle-aged with elevated waist circumference and late-night cravings. After protein-first breakfasts, 20 minutes of daily walking, and breathing exercises, they reported reduced cravings and improved BP.
Patient B: Young professional with mood variability and afternoon crashes. Polyphenol-rich lunches, magnesium supplementation, and sleep regularization improved mood and productivity.
Patient C: Long-term alcohol use, “zero-carb” belief. Gradual reduction, hydration, and evening routine improved sleep, reduced cravings, and stabilized weight.
These cases illustrate how multi-system alignment produces results that patients can feel and sustain.
Advanced Laboratory Considerations
For select patients:
hs-CRP, IL-6, TNF-α: inflammation markers
Tryptophan, kynurenine, and ratio assessments
Lipid panel, fasting insulin, HOMA-IR
Sleep study for suspected apnea
HRV tracking for autonomic insights
Rationale: Identifies contributors to IDO activation, insulin resistance, and autonomic imbalance.
Precision Supplementation: Principles and Cautions
Omega-3 EPA/DHA for mood and endothelial support
Magnesium glycinate for sleep and vascular tone
B-complex with methylated folate/B12 for monoamine synthesis
Polyphenols (EGCG, resveratrol) for inflammatory modulation
Creatine for neurometabolic support and cognitive resilience
Always personalized based on medical history and labs. Supplements support, but do not replace, behavioral foundations.
Integration with Care Teams: Nursing, Nutrition, and Coaching
The best outcomes arise from interdisciplinary collaboration—nursing assessments, nutrition counseling, and health coaching reinforce habit adherence and monitor progress. Communication enhances implementation fidelity and patient experience.
Community and Culture: Social Reinforcement
Group-based programs harness social reward and accountability. Community meals, walking clubs, and digital support tools align dopamine signaling with healthy behaviors.
Performance Layer: Cognitive and Physical Capacity
Nutrition timing enhances sustained focus
Strength training improves resilience and metabolic reserve
Strategic breaks prevent decision fatigue
Sleep protects working memory and creative problem-solving
Outcome: A brain-body platform for long-term success.
Reinforce changes through the environment and the community
The approach is integrative, evidence-based, and patient-centered.
Summary
This educational post presents an integrated, evidence-based framework linking striatal dopamine signaling, serotonergic metabolism, inflammatory pathways, autonomic regulation, and gut-brain interactions to practical strategies for obesity, mood regulation, and performance. Reductions in D2 receptor availability are associated with compulsive eating and reward dysregulation; structured interventions—such as protein-first nutrition, sleep optimization, and progressive exercise—enhance receptor sensitivity and stabilize cravings. Inflammation-driven IDO activation diverts tryptophan from serotonin to kynurenine metabolites, contributing to mood symptoms and fatigue; anti-inflammatory nutrition, micronutrient support, and physical activity rebalance this axis. Autonomic strategies—breathing, movement, sleep hygiene—improve blood pressure and endothelial function. Behavioral architecture (ABCs) embeds habits within basal ganglia circuits, translating physiological principles into daily practice. Clarifying misconceptions about “zero-carb alcohol” highlights how reward circuitry and hepatic metabolism complicate health goals. The overall map aligns neurochemistry, lifestyle, and personalization for sustainable outcomes.
Conclusion
Metabolic health, mood, and performance are inseparable dimensions of neuroendocrine physiology. By recognizing how the striatum, serotonin pathways, IDO–kynurenine axis, and autonomic balance respond to nutrition, stress, sleep, and movement, we can deploy targeted interventions that recalibrate reward sensitivity and emotional stability. Patients thrive when care is layered: food-first strategies, structured exercise, sleep architecture, stress modulation, and precision supplementation when indicated. This integrative method is not about perfection but consistency, building small victories that rewire habit circuits and restore resilience. As clinicians and patients collaborate—guided by data and behaviors that feel achievable—the brain-body system gradually shifts from reactivity to regulation, enabling healthy weight management, improved mood, and better performance.
Key Insights
Dopamine D2 receptor downregulation in the striatum contributes to obesity and compulsive eating; exercise, sleep, and protein-first strategies improve reward sensitivity.
Inflammation activates IDO, diverting tryptophan from serotonin to kynurenine, which can impair mood and energy; anti-inflammatory nutrition, micronutrients, and physical activity rebalance pathways.
Autonomic interventions—such as slow breathing, aerobic and resistance exercise, and sleep optimization—lower blood pressure and support endothelial health.
Gut-brain integration: omega-3s, fiber, and polyphenols modulate inflammation and neurotransmitter signaling; microbiome health strengthens the gut barrier and reduces systemic inflammation.
The behavior change framework (ABCs) embeds habits into neural circuits, reducing decision fatigue and sustaining progress.
Alcohol is not metabolically neutral—even low-carb spirits disrupt reward circuits, sleep, and hepatic metabolism, often undermining goals.
Personalization via data—tracking waist circumference, BP, HRV, sleep, and mood—guides targeted adjustments and reinforces adherence.
References
Volkow ND, Wang G-J, Fowler JS, Telang F. Overlapping neuronal circuits in addiction and obesity: evidence of systems pathology. Biol Psychiatry.
Wang G-J et al. Brain dopamine and obesity. Lancet.
Cervenka S et al. Imaging of dopamine receptors in obesity. Int J Obes.
Raison CL, Capuron L, Miller AH. Cytokines sing the blues: inflammation and the pathogenesis of depression. Trends Immunol.
Schwarcz R, Stone TW. The kynurenine pathway and neurodegenerative disease. J Neurochem.
Pedersen BK. The diseasome of physical inactivity—and the role of myokines. Exp Clin Endocrinol Diabetes.
Brook RD et al. Beyond medications and diet: alternative approaches to lowering blood pressure. Hypertension.
Walker MP. The role of sleep in cognition and emotion. Ann NY Acad Sci.
Vercambre M-N et al. Polyphenols and vascular function. Nutrients.
Young SN. Tryptophan, 5-HT, and mood. J Psychiatry Neurosci.
He FJ, MacGregor GA. Salt intake and BP. Lancet.
Mozaffarian D et al. Omega-3s and cardiovascular health. Circulation.
Brewer JA. Mindfulness and reward processing. Ann NY Acad Sci.
Disclaimer: This educational content is for informational purposes only and should not be used as medical advice. All individuals must obtain recommendations for their personal situations from their own medical providers.
A hand clinging to the rock during a sport climbing session.
How ChiroMed’s Integrative Chiropractic Care in El Paso, TX, Prevents Future Injuries in Athletes Using Functional Movement Assessments
Athletes in El Paso, TX, often train hard to reach their goals, but small body issues can build up and cause injuries that sideline them. At ChiroMed – Integrated Medicine Holistic Healthcare, located at 11860 Vista Del Sol, Suite 128, athletes can get ahead of these problems with functional movement assessments. This approach spots hidden imbalances like tight muscles, weak spots, or stiff joints before pain hits. Our team, led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, uses adjustments, soft-tissue therapies, and targeted exercises to address these issues, boost nervous system function, improve body mechanics, and prevent overuse injuries.
Functional movement assessments at ChiroMed check how your body moves during sports and daily tasks. These tests assess balance, flexibility, strength, and coordination. Simple actions such as squats, steps, or arm reaches help reveal where movements are off. Even without pain, these assessments find subclinical imbalances—minor problems that could turn into big injuries later. Our El Paso experts use these tools to create a plan tailored to each athlete’s needs.
Detecting uneven posture or weight shifts that strain one side
Finding limited motion in key areas like the hips or the shoulders
Spotting weak muscles in the core or legs that affect stability
Noting tight spots that throw off joint alignment
ChiroMed’s integrative chiropractic care blends spinal adjustments, soft-tissue work, and corrective exercises to address these findings. Adjustments gently realign joints to ease nerve pressure and improve signals throughout the body. Soft tissue therapies, such as massage or specialized tools, release tension and help heal old scars. Corrective exercises then strengthen weak areas and teach better movement habits. This holistic method enhances nerve function, refines biomechanics, and prevents the body from compensating in ways that lead to injuries.
The nervous system is key to muscle control. Misalignments can disrupt signals, causing poor coordination or delayed responses. At ChiroMed in El Paso, TX, our adjustments clear these blocks, helping muscles work together smoothly. Better biomechanics allow joints to move freely without extra wear, protecting areas like knees, backs, and ankles from stress.
Compensation patterns develop when the body overuses strong areas to cover for weak ones. For instance, runners with pelvic tilts might strain their knees or shins. Swimmers or lifters with poor shoulder form could overload muscles and cause tears. ChiroMed’s team corrects these early to keep athletes training safely.
Common subclinical imbalances we identify at ChiroMed through functional movement assessments include:
Tension in the back or legs that limits bending or twisting
Weak hip muscles that make the body unstable during runs or jumps
Stiff ankles that alter how you walk or land
Uneven arm mobility that impacts throws or lifts
Shaky core strength leading to back strain in heavy activities
Addressing these at our El Paso clinic lowers injury risks and supports steady training. Regular sessions also mean faster fixes for any small setbacks, reducing time away from sports.
Our process starts with a full review of your history and a hands-on exam. We observe your movements and note any uneven patterns. From there, we build a custom plan. Adjustments fix spinal alignment, soft tissue work eases restrictions, and exercises reinforce strength. Over time, this improves your balance, flexibility, speed, and endurance.
Key benefits of ChiroMed’s functional movement assessments and integrative care:
Lower risks of twists, pulls, inflammation, or breaks
Greater joint range and muscle stretch for top performance
Quicker reflexes from improved nerve signals
Less swelling and faster bounce-back after sessions
Extended active years by avoiding long-term wear
Runners visiting ChiroMed often have pelvic imbalances that affect their gait. Our adjustments and core-strengthening exercises level things out, making runs smoother and safer. Lifters with tight shoulders might arch their backs wrongly, risking strain—our therapies and drills fix that before issues arise.
Contact sports players benefit from our spinal checks to better absorb hits. Swimmers get help with shoulder flow to avoid overuse. Even casual gym-goers in El Paso see better stamina and less aching. ChiroMed’s methods suit all levels by proactively targeting root problems.
Dr. Alexander Jimenez, DC, APRN, FNP-BC, leads ChiroMed with his expertise in chiropractic, family nursing, and functional medicine. His clinical observations show that combining assessments with adjustments, nutrition, and rehab effectively treats sports injuries, nerve pain, and body imbalances. At ChiroMed, Dr. Jimenez focuses on non-invasive care that reduces inflammation, restores motion, and prevents reoccurrences. His El Paso practice integrates these elements to boost performance, ease chronic discomfort, and promote overall health.
This interconnected approach views the body as a whole system. A restriction in one spot can ripple through others. ChiroMed breaks these chains by realigning and teaching lasting habits.
Additional advantages athletes experience at ChiroMed include:
Straighter posture for everyday and athletic tasks
Sharper body sense for secure movements and changes
Reduced tiredness in extended workouts
Stronger output from smooth mechanics
Mental sharpness from fewer distractions
Our preventive care in El Paso saves athletes from costly fixes or lost events. Many report feeling more balanced, powerful, and assured after our programs.
To sustain gains, we recommend ongoing visits based on your sport and load. High-intensity athletes might come weekly, while others come monthly. Home exercises keep progress going.
We also educate on warm-ups, stretches, and sport-specific form. Nutrition tips help repair and reduce swelling. Teaming with trainers or therapists rounds out support.
ChiroMed also offers nurse practitioner services, naturopathy, and rehab for full holistic care. Whether you’re a pro or a hobbyist in El Paso, our team helps you move better and stay injury-free.
Injuries can derail plans, but ChiroMed’s approach catches them early. We blend modern assessments with proven therapies to optimize your body.
Athletes trust us for personalized plans that fit their lives. From initial scan to follow-ups, we guide you toward peak health.
In conclusion, at ChiroMed – Integrated Medicine Holistic Healthcare in El Paso, TX, functional movement assessments help spot subclinical imbalances before pain starts. Our integrative chiropractic care—with adjustments, soft-tissue work, and exercises—boosts nerve function, optimizes biomechanics, and halts harmful patterns. Runners fix pelvic tilts, lifters correct techniques, and all athletes train uninterrupted. Contact us at (915) 850-0900 to prevent injuries and enhance your game.
A young girl does hyperextension exercises to improve back muscles and core strength
A back extension machine—often called a hyperextension bench or Roman chair—is a common gym tool used to train the posterior chain, meaning the muscles along the back side of your body. When it’s set up correctly and used with controlled form, it can help build core stability, strengthen the erector spinae (the long muscle group that runs along your spine), and support better movement patterns for daily life and training.
This matters because a “strong core” is not only about visible abs. It also includes the muscles that support the spine and help you stay stable while lifting, carrying, bending, and twisting. When the posterior chain is weak or poorly coordinated, people often compensate with poor mechanics, which can lead to recurring discomfort over time.
That said, back extensions are not a “push through pain” exercise. They should feel like muscle work, not sharp pain, pinching, or electric symptoms down the leg. If symptoms feel nerve-like, or if you have a known spine condition, it’s smart to get guidance from a qualified clinician before loading this movement.
What the Back Extension Machine Does (and Why It Works)
Most back extension machines are built so you can hinge at the hips while your feet and lower legs are supported. Your torso lowers forward, then extends back up smoothly and in control. This trains the body to produce force through the hips while the trunk stays braced.
Seated back extension machine with a weight stack (you sit and extend backward against resistance)
Main muscles trained
Back extensions can activate several important muscles, including:
Erector spinae (spinal extensors that help you stay upright)
Glutes (hip extension and pelvic support)
Hamstrings (assist hip extension and control the lowering phase)
Deep core stabilizers (bracing to keep the spine steady)
Some equipment is also designed to be adjustable, so you can change the pad position and body angle. This can shift emphasis slightly between the lower back and hips.
Quick Setup: How to Adjust the Pads and Foot Holds
Good setup is not optional—it’s the difference between a safe hip hinge and an awkward spine bend.
Use these checkpoints:
Hip pad height: The top of the pad should sit at or just below the front of your hip bones so your hips can hinge freely.
Feet secured: Heels supported and feet locked into the restraints so you feel stable before you move.
Body line: At the top position, aim for a straight line from head to tailbone (not a “crunched” posture).
Machine adjustability: If you’re using an adjustable unit, choose a setting that fits your leg length and hip position (many benches offer multiple pad angles/heights).
A simple clue: if you feel like you’re bending mostly through the low back instead of hinging through the hips, your setup is probably off.
Step-by-Step: How to Do Back Extensions with Neutral-Spine Form
Below is a clear, repeatable method that works for most healthy lifters using bodyweight or a light load.
Brace before you move
Set your feet and hips as described above.
Cross your arms over your chest (or put your hands at your sides if you already have strong control).
Take a breath and gently brace your midsection like you’re preparing to be bumped.
Hinge down (controlled lowering)
Think: “hips back”, not “round forward.”
Lower your torso until you feel a strong stretch in the hamstrings and glutes.
Keep the neck neutral (eyes looking slightly down).
Drive up with glutes and hamstrings
Squeeze your glutes and bring your torso back up.
Stop when your body is straight (neutral), not leaning back.
Avoid hyperextension at the top
The finish is “tall and braced,” not “arched hard.”
If you feel low-back compression at the top, reduce the range or lighten the load.
WebMD also describes back extensions as a movement pattern that should be approached with attention to form and comfort, especially when people use extension-based exercises for their backs.
Common Mistakes (and Easy Fixes)
These are some of the most common issues seen in the gym and in rehab-style strength work.
Mistake: Bending through the lower back instead of hinging at the hips Fix: Adjust the pad so the hips can hinge freely; keep ribs “down” and brace.
Mistake: Swinging or using momentum Fix: Slow down the lowering phase (2–3 seconds down) and pause briefly.
Mistake: Hyperextending at the top Fix: Stop at neutral alignment; think “straight line,” not “lean back.”
Mistake: Going too heavy too soon Fix: Start with body weight and perfect control, then gradually add load.
Smart Programming: Sets, Reps, and Progression
A back extension machine can be used for strength, stability, or rehab-style rebuilding—depending on how you program it.
Beginner (control + tolerance)
2–3 sets of 8–12 reps
Bodyweight only
Rest 60–90 seconds
General fitness (posterior chain support)
3 sets of 10–15 reps
Add a small plate or dumbbell hugged to the chest if form stays clean
Strength focus (only if form is rock-solid)
3–5 sets of 6–10 reps
Heavier load, slower tempo
Stop sets before form breaks down
A practical equipment note: many Roman chair benches and back extension units are adjustable to accommodate different body sizes and training angles, helping people find a safer hinge position.
When to Be Careful (Red Flags and Modifications)
Back extensions are not for “everyone, all the time.” Use extra caution or professional guidance if you have:
Pain that shoots down the leg, numbness, tingling, or weakness
A known disc injury that flares with extension-based movements
New or worsening pain after starting the movement
History of significant spine trauma
Options that may be safer (depending on the person) include:
Shorter range of motion
Isometric holds in a neutral position
Glute-focused hip extension variations where the spine stays braced
On Dr. Alexander Jimenez’s site, hyperextension is discussed as a movement that can help strengthen muscles but should be matched to the person’s needs, especially when low back pain is involved. The key theme is using exercise alongside appropriate clinical care and progressions.
How Integrative Chiropractic Care and Nurse Practitioners Can Complement Back Extensions
Strength work is powerful—but many people do best with a complete plan, not a single exercise.
Chiropractic care: improving motion and reducing irritation
In an integrative setting, chiropractic care may focus on:
Restoring joint motion and spinal mechanics
Reducing stiffness that changes hinge patterns
Supporting better movement timing between the hips, pelvis, and spine
Some chiropractic sources also describe a whole-person approach that pairs adjustments with movement habits and supportive care.
Nurse practitioner support: whole-body factors that affect pain and healing
Nurse practitioners (NPs) often add value by addressing factors that can keep people “stuck,” such as:
Sleep, stress load, and recovery capacity
Inflammation drivers and nutrition basics
Medication review and safer pain-management planning when appropriate
Screening for red flags that require imaging or referral
In other words, exercise strengthens tissue capacity, while clinical oversight helps remove barriers that sustain pain patterns.
The integrative “bridge” between rehab and performance
A practical integrated approach often looks like this:
Improve movement quality first (mobility + hinge mechanics)
Build strength with controlled exercises (like back extensions)
Progress to more demanding patterns (lifting, carrying, athletic training)
This “combined plan” concept—pairing adjustments, targeted exercise, and individualized care—is also described in integrated therapy-style chiropractic articles focused on building a personalized plan that includes spinal work and strengthening.
Clinical Observations from Dr. Alexander Jimenez, DC, APRN, FNP-BC
Across Dr. Jimenez’s educational content, a consistent clinical message is that many back-pain patterns are not solved by a single tool. People tend to do better when they:
Restore motion where it is limited
Reinforce stability and strength where it is weak
Progress exercise choices based on symptoms and tolerance (not ego)
Combine training with clinical evaluation when pain persists
His hyperextension-focused series emphasizes how extension-related patterns can connect to low back symptoms and how exercise progressions may support strengthening when used appropriately.
He also discusses core- and squat-related strengthening as part of a broader strategy for back and hip function—important because hip strength and trunk control are major parts of how a back extension machine should be performed (hinge + brace).
Putting It All Together: A Simple, Comprehensive Plan
Here’s a clean way to combine gym training with integrative clinical care.
Step 1: Reset the basics (1–2 weeks)
Gentle mobility for hips and mid-back
Short-range back extensions (bodyweight only)
Focus on bracing and controlled tempo
Step 2: Build capacity (3–6 weeks)
Increase back extension reps slowly (example: add 1–2 reps per week)
Add glute and hamstring accessories (bridges, hinges, split squats)
Add walking or light conditioning for circulation and recovery
Step 3: Progress to real-world strength (ongoing)
Add load to back extensions only if the neutral form is automatic
Transition strength to compound lifts and carries when appropriate
Maintain a weekly “spine hygiene” routine (mobility + stability)
If pain is persistent or complex, the integrative model is often used to evaluate movement, address joint mechanics and irritation, strengthen intelligently, and support recovery systems.
Key Takeaways
The back extension machine (Roman chair/hyperextension bench) strengthens the erector spinae, glutes, and hamstrings, supporting core stability when done with control.
Proper setup matters: align the pad for a true hip hinge, brace the core, and avoid “cranking” into the low back.
The goal is neutral at the top, not hyperextension.
Integrative care can help by improving motion, reducing irritation, and guiding progressions—while NPs support recovery, whole-body drivers, and safety screening.