
Hip Injuries After Car Accidents
ChiroMed’s Integrated Recovery Approach
A motor vehicle accident can place extreme force on the hip joint. Even when a crash looks “minor,” the body can absorb a strong impact in only a few seconds. The knee may hit the dashboard. The foot may press hard into the floorboard. The seatbelt may lock across the pelvis. The body may twist while the hip is fixed in place.
The hip is one of the strongest joints in the body. It is built for stability, walking, standing, lifting, and balance. Because it is so stable, serious hip injuries usually take a high-energy force. That is why hip pain after a car accident should be taken seriously.
At ChiroMed, the focus is on helping patients understand the injury, document the damage, reduce pain, restore movement, and rebuild function. For car accident patients in El Paso, Texas, this often means combining chiropractic care, medical oversight, personal injury care, functional medicine, rehabilitation, and advanced recovery options when appropriate.
Why the Hip Is Vulnerable During a Crash
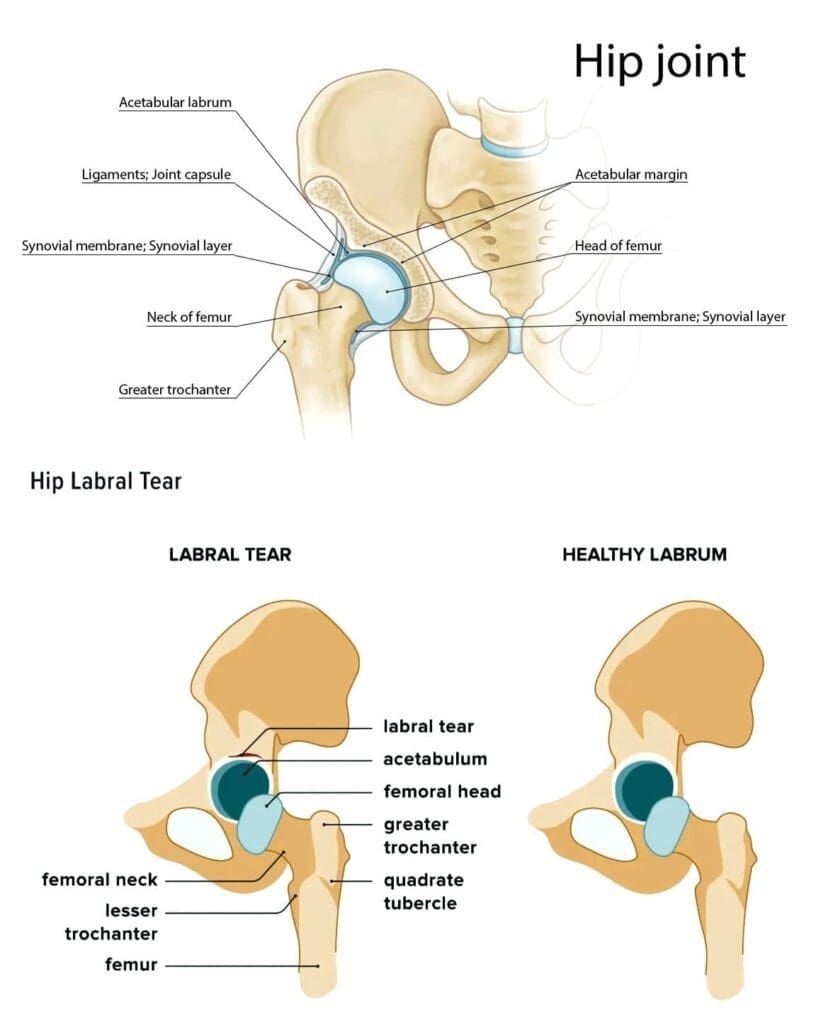
The hip is a ball-and-socket joint. The “ball” is the femoral head at the top of the thighbone. The “socket” is the acetabulum, which is part of the pelvis. Around the joint are muscles, tendons, ligaments, cartilage, and the labrum. These structures work together to keep the hip strong, stable, and mobile.
During a crash, force can travel quickly through the lower body. A common example is the dashboard injury. This can happen when the knee strikes the dashboard, driving the thighbone backward. That force can push the ball of the hip out of the socket, causing a hip dislocation. In some cases, the same force can also fracture the hip socket or damage the femoral head (American Academy of Orthopaedic Surgeons [AAOS], n.d.-a; Masiewicz & Johnson, 2023).
Hip injuries may also happen when:
- The driver or passenger braces against the floorboard
- The pelvis is trapped by the seatbelt during impact
- The body twists while the leg is planted
- The hip hits the door, console, or seat frame
- The crash causes sudden rotation through the pelvis and lower back
The position of the legs and body during the crash can affect the type of injury. A bent hip and knee may increase the risk of a dashboard-type injury. A side impact may create direct trauma to the outside of the hip. Sudden twisting may injure the labrum, tendons, ligaments, or surrounding muscles.
Common Hip Injuries After Motor Vehicle Accidents
Hip injuries after a car accident can range from mild to severe. Some patients have muscle soreness that improves with care. Others may have a fracture, dislocation, or deep joint injury that needs urgent medical attention.
Hip Dislocation
A hip dislocation happens when the ball of the thighbone is forced out of the socket. This is a serious injury and requires immediate medical care.
Motor vehicle accidents are one of the most common causes of traumatic hip dislocations. The classic crash pattern occurs when the knee hits the dashboard, driving force through the thighbone into the hip joint (AAOS, n.d.-a).
Signs of a hip dislocation may include:
- Severe hip or groin pain
- Inability to stand or walk
- A leg that looks shortened or turned inward
- Severe pain with movement
- Numbness, tingling, or weakness
- Visible deformity around the hip or leg
A dislocated hip may also damage blood vessels, nerves, cartilage, and bone. The joint usually needs to be reduced, meaning the ball must be placed back into the socket by trained medical professionals. Imaging is often needed to check for fractures and other damage.
Acetabular Fracture
An acetabular fracture is a break in the socket part of the hip joint. These fractures often happen from high-energy trauma, including motor vehicle accidents. The femoral head may be driven into the socket with enough force to crack or break the pelvis (AAOS, n.d.-b).
This injury can be serious because the hip socket must stay smooth and stable for normal movement. If the socket heals in a poor position, the patient may develop long-term pain, stiffness, arthritis, or difficulty walking.
Symptoms may include:
- Deep hip or groin pain
- Pain with weight-bearing
- Swelling or bruising
- Trouble moving the leg
- Numbness or weakness if nerves are involved
Some acetabular fractures may be treated without surgery if the joint is stable. More severe fractures may require surgery to restore the normal shape of the hip socket.
Femoral Head Fracture
The femoral head is the ball at the top of the thighbone. A femoral head fracture can happen when the ball is crushed against the socket during a crash. This injury may occur with a hip dislocation, creating a fracture-dislocation.
This type of injury needs careful evaluation because the femoral head carries body weight. Damage to this area can affect walking, joint motion, cartilage health, and long-term hip function.
Patients may feel:
- Severe hip pain
- Groin pain
- Trouble standing
- Limited range of motion
- Pain deep inside the joint
A femoral head fracture should be evaluated with imaging and orthopedic care.
Hip Labral Tear
The labrum is a ring of cartilage that lines the hip socket. It helps deepen the socket and keep the joint stable. A labral tear can occur when the hip is twisted, compressed, dislocated, or forced into an abnormal position during a crash.
Mayo Clinic notes that trauma, including injury or dislocation from a car accident, can cause a hip labral tear (Mayo Clinic, 2024).
Symptoms may include:
- Hip or groin pain
- Clicking, locking, or catching in the hip
- Stiffness
- Pain with sitting, walking, or pivoting
- Reduced range of motion
- A feeling that the hip is unstable
Labral tears can be hard to detect without the right exam and imaging. Some patients may feel pain right away. Others may notice symptoms days or weeks after the crash.
Muscle Strains and Ligament Sprains
Not all hip injuries are fractures or dislocations. Many accident-related hip problems involve soft tissue damage. This can include strained muscles, sprained ligaments, irritated tendons, and inflamed bursae.
Common soft tissue injuries include:
- Hip flexor strain
- Hamstring strain
- Gluteal strain
- Ligament sprain
- Trochanteric bursitis
- Deep bruising
- Sacroiliac joint irritation
- Pelvic muscle guarding
These injuries may not look dramatic on the outside, but they can still cause major pain. A person may limp, avoid stairs, struggle to sit, or feel pain when getting in and out of a car.
Why Hip Pain May Show Up Later
After an accident, adrenaline can hide pain. Some people feel “okay” at first, then wake up the next day with stiffness, swelling, bruising, or deep hip pain. This delayed pain does not mean the injury is fake or minor.
Pain may show up later because of:
- Inflammation
- Muscle guarding
- Joint swelling
- Bruising
- Labral irritation
- Nerve irritation
- Changes in walking pattern
- Pelvic or low back compensation
Delayed-onset hip pain after a car accident should be evaluated, especially when it affects walking, standing, sitting, or daily activities.
How ChiroMed Looks at Hip Injuries After Accidents
ChiroMed’s approach is built around the idea that car accident injuries are often connected. A painful hip may also involve the low back, pelvis, sacroiliac joints, knees, muscles, nerves, and movement patterns.
For this reason, care should not focus only on the painful spot. A full evaluation may look at:
- Hip range of motion
- Pelvic alignment
- Low back movement
- Walking pattern
- Strength and stability
- Muscle tightness
- Nerve signs
- Pain triggers
- Functional limits
- Need for imaging or referral
This whole-body view helps create a safer and more complete recovery plan.
Chiropractic Care for Hip, Pelvis, and Spine Function
After a crash, the body may protect the injured hip by altering its movement. A person may limp, shift weight to one side, tighten the lower back, or rotate the pelvis. These changes can create new pain patterns.
Chiropractic care may help improve motion in the spine, pelvis, sacroiliac joints, and surrounding structures. The goal is not to force the hip through pain. The goal is to restore better movement, reduce mechanical stress, and help the body move with less compensation.
Chiropractic care may support:
- Pelvic balance
- Lumbar spine mobility
- Sacroiliac joint motion
- Hip mechanics
- Reduced muscle guarding
- Better posture
- Improved walking patterns
For accident patients, this care may also be paired with rehabilitation and medical oversight.
Medical Oversight With Dr. Maria Guadalupe Cardenas, MD
At Injury Medical Clinic PA, the multidisciplinary model includes medical direction from Dr. Maria Guadalupe Cardenas, MD, Board Certified in Internal Medicine. Dr. Cardenas serves as the Medical Director and Collaborative Physician, working with Dr. Alex Jimenez, DC, in an integrative injury care setting in El Paso, Texas.
Dr. Cardenas is listed with NPI #1164426749 and Texas MD License #J2933. With over 40 years of experience as an internist, she brings medical oversight to a clinic model that combines chiropractic care, rehabilitation, personal injury care, functional medicine, and related services.
This type of structure is common in integrative and injury care clinics. The chiropractor focuses on structural and functional recovery, while the medical director supports safe medical protocols, clinical direction, and coordinated care.
Medical oversight is especially important when patients have:
- Severe trauma
- Possible fractures or dislocations
- Diabetes
- High blood pressure
- Heart disease
- Medication concerns
- Chronic inflammation
- Complex pain
- Older age
- Need for referral or imaging
This team-based model helps support patient safety and better care planning.
Dr. Alex Jimenez’s Clinical Observations
Dr. Alexander Jimenez, DC, APRN, FNP-BC, CCST, CFMP, IFMCP, ATN, has long emphasized that injury care should look beyond the surface symptom. In his clinical observations, hip pain after a motor vehicle accident often involves a chain reaction through the pelvis, low back, knees, and nervous system.
A hip injury can change the way a person walks. That change can stress the lower back. Low back irritation can then affect the hip and leg. This cycle can make recovery slower if the full pattern is not addressed.
At ChiroMed, this supports a more complete care path that may include:
- Structural evaluation
- Chiropractic care
- Functional movement testing
- Rehabilitation
- Soft tissue support
- Personal injury documentation
- Functional medicine support
- Medical oversight
- Regenerative therapy discussion when appropriate
The goal is to help the patient move better, heal better, and return to daily life with more confidence.
Rehabilitation: Restoring Strength and Mobility
Rehabilitation is one of the most important parts of hip recovery after a crash. Once serious injuries are ruled out and the patient is medically stable, rehab can help restore motion, strength, and balance.
A hip rehab plan may include:
- Gentle stretching
- Range-of-motion exercises
- Glute strengthening
- Hip flexor control
- Core stability
- Balance training
- Walking retraining
- Pelvic stabilization
- Gradual return to normal activity
Rehab should progress at the right speed. Moving too fast may irritate the injury. Moving too little may cause stiffness and weakness. The right plan helps the hip regain safe function step by step.
Regenerative Therapies for Selected Hip Injuries
Some patients may be candidates for regenerative therapies such as PRP, PFP, or MFAT. These options are not emergency treatments for fractures or dislocations. They do not replace surgery when surgery is needed. However, they may be considered for selected soft tissue injuries, tendon problems, joint irritation, or ongoing pain when appropriate.
PRP stands for platelet-rich plasma. It uses a patient’s own blood, which is processed to concentrate platelets. Platelets contain growth factors that may help regulate inflammation and support tissue repair. Research on PRP for hip conditions is still developing, but some studies suggest it may help reduce pain and improve function in selected hip conditions (Kraeutler et al., 2016; Lim et al., 2023).
PFP refers to platelet-rich plasma/fibrin products. Fibrin may act like a natural scaffold that helps keep healing signals in the area longer.
MFAT stands for microfragmented adipose tissue. This therapy uses processed fat tissue that contains cells and signaling factors that may support repair and reduce inflammation. Research on MFAT for hip osteoarthritis and related joint problems is promising, but still developing (Natali et al., 2022).
These options should always be discussed with a qualified medical provider to determine whether they are appropriate for the patient’s injury, health history, and goals.
When Hip Pain Needs Immediate Attention
Some symptoms after a car accident should not wait.
Seek urgent medical care for:
- Severe hip pain
- Inability to stand or walk
- A leg that looks twisted or shortened
- Numbness or weakness
- Major swelling or bruising
- Deep groin pain after a crash
- Pain after a high-speed impact
- Loss of bladder or bowel control
- Suspected dislocation or fracture
Early evaluation can help protect the hip joint and reduce the risk of long-term problems.
A Better Path Forward After an Accident
Hip injuries after motor vehicle accidents can affect every part of daily life. Walking, sitting, sleeping, working, and driving may all become painful. Some injuries heal with conservative care. Others need imaging, medical referral, injections, or surgery.
The most important step is getting the right evaluation early.
At ChiroMed, the goal is to help accident patients understand their injuries and receive care that supports healing, function, and proper documentation. With chiropractic care from Dr. Alex Jimenez, medical oversight from Dr. Maria Guadalupe Cardenas, MD, and a multidisciplinary approach that includes rehabilitation, functional medicine, personal injury care, and regenerative options when appropriate, patients can receive a more complete path toward recovery.
The hip carries the body forward. After a crash, the right care plan can help restore strength, stability, and movement one step at a time.
References
American Academy of Orthopaedic Surgeons. (n.d.-a). Hip dislocation. OrthoInfo.
American Academy of Orthopaedic Surgeons. (n.d.-b). Acetabular fractures. OrthoInfo.
Ammori, M. B., et al. (2018). The biomechanics of lower limb injuries in frontal-impact road traffic collisions. Journal of Orthopaedics and Traumatology.
Jimenez, A. (n.d.). Dr. Alex Jimenez, DC, APRN, FNP-BC.
Jimenez, A. (n.d.). Dr. Alexander Jimenez DC, APRN, FNP-BC, IFMCP, CFMP, ATN. LinkedIn.
Kraeutler, M. J., Chahla, J., & LaPrade, R. F. (2016). The use of platelet-rich plasma to augment conservative and surgical treatment of hip and pelvic disorders. Orthopedic Reviews.
Lim, A., et al. (2023). The use of intra-articular platelet-rich plasma as a therapeutic intervention for hip osteoarthritis. Orthopaedic Journal of Sports Medicine.
Masiewicz, S., & Johnson, D. (2023). Posterior hip dislocation. StatPearls. StatPearls Publishing.
Mayo Clinic. (2024). Hip labral tear: Symptoms and causes.
Natali, S., et al. (2022). Is intra-articular injection of autologous micro-fragmented adipose tissue effective in hip osteoarthritis?. Journal of Clinical Medicine.


















