Effective Rehabilitation Exercises for Head Injuries: A Guide to Restoring Skills
Head injuries can happen from falls, car accidents, or sports. They range from mild concussions to more serious traumatic brain injury (TBI). These injuries often impact a person’s ability to move, think, and maintain balance. Recovery takes time and effort. Rehabilitation exercises play a significant role in helping people regain their physical, cognitive, and balance skills. These exercises combine aerobic activities, strength training, balance exercises, and cognitive tasks to provide a comprehensive workout. They help the brain heal by forming new connections, a process known as neuroplasticity. In this article, we will examine various types of exercises and their benefits. We will also discuss how chiropractic care can support the recovery process. Always consult a doctor before starting any exercise program.
What Are Head Injuries and Why Do We Need Rehabilitation?
A head injury occurs when the brain gets bumped or shaken inside the skull. This can cause swelling, bleeding, or damage to brain cells. Symptoms might include headaches, dizziness, memory problems, or trouble walking. Traumatic brain injury is a common type of head injury. It affects millions of people each year. Recovery depends on the severity of the injury and the promptness of treatment initiation.
Rehabilitation helps restore lost skills. It utilizes exercises to strengthen the body and brain. Physical exercise builds muscle and improves movement. Cognitive exercises sharpen thinking and memory. Balance exercises prevent falls. Starting slow is key. Even simple activities, such as walking, can help. As you improve, exercises can become more challenging. The goal is to make daily life easier and safer.
Experts say that early rehabilitation can reduce hospital time and enhance independence. Delays might lead to lasting problems. That’s why exercises should start as soon as it’s safe. They improve blood flow to the brain, which brings oxygen and nutrients for healing. They also lift mood and fight fatigue.
Physical Exercises: Building Strength and Endurance
Physical exercises are a main part of rehab for head injuries. They focus on aerobic and strength activities. Aerobic exercises get the heart pumping. They include low-impact things like walking or swimming. Strength exercises, such as squats or rows, build muscle. These help restore movement and prevent weakness.
Aerobic Exercises
Aerobic activities are great for heart health and brain recovery. They increase blood flow, which helps the brain heal. Guidelines suggest 150 minutes of moderate aerobic exercise per week. Break it into short sessions, like 10 minutes at a time. Examples include:
Walking: Start slow on flat ground. As you improve, add hills or speed. This helps build endurance and aids with daily tasks.
Cycling: Use a stationary bike if balance is an issue. Pedal for 20-30 minutes. It strengthens legs without much impact.
Swimming: Water supports the body, making it easier on joints. Swim laps or do water aerobics. This improves breathing and muscle tone.
Do these 3-5 times a week. Keep intensity moderate – you should be able to talk but not sing. If you feel dizzy, stop and rest.
Strength Training Exercises
Strength training fights muscle loss after a head injury. It targets arms, legs, and core. Use body weight or light weights. Do 2 sessions a week with 8-12 reps per exercise. Examples include:
Squats: Stand with feet shoulder-width apart. Bend your knees as if sitting in a chair, then stand up. This strengthens legs and helps with standing.
Rows: Sit or stand. Pull your elbows back like rowing a boat. Use a band or weights. It builds back muscles for better posture.
Bicep Curls: Hold a water bottle. Bend your elbow to bring it to your shoulder, then lower. Do 10 times per arm. This improves arm strength for daily tasks.
Straight Leg Raises: Lie on your back. Lift one leg straight up, hold it, then lower it. This targets thigh muscles.
These exercises use neuroplasticity to rewire the brain. Repeat them often to build new pathways. Start with help if needed.
Arm exercises are important too. They assist with tasks such as eating and dressing. Try pushing a water bottle across a table. Or do shoulder flexion: Lift your arm straight in front to eye level. Hold for 5 seconds. These restore arm function and coordination.
Leg exercises build a strong base. Seated marching: Lift one knee at a time while sitting. Or hip abduction: Kick one leg out to the side. These exercises improve walking and reduce the risk of falls.
Core exercises support the whole body. Try oblique crunches: Dip one shoulder toward the opposite hip. Or forward punches: Punch out while leaning forward. A strong core helps with balance and posture.
Balance Exercises: Staying Steady on Your Feet
Balance problems are common after traumatic brain injury. They result from damage to the inner ear or brain areas that control balance and stability. Balance exercises help train the body to maintain its upright position. They reduce dizziness and prevent falls.
Start with simple stances. Tandem stance: Put one foot in front of the other, like on a tightrope. Hold for 30 seconds. Switch feet. Do this with your eyes open, then close them for a more challenging experience. It improves proprioception – the sense of where your body is in relation to its surroundings.
Weight shifts: Stand with feet apart. Shift your weight to one side and lift the other foot slightly. Hold 30 seconds. This builds stability.
Romberg stance: Stand with feet together, eyes closed. Hold as long as you can. It forces the brain to use other senses for balance.
Heel-toe raises: Rise on toes, then rock back on heels. Alternate. This strengthens calves and improves gait.
Advanced exercises include standing on one leg or walking on different surfaces. Use a chair for support at first. Vestibular rehabilitation adds head and eye movements to help combat dizziness. For example, gaze stabilization: Focus on a point while turning your head.
Do balance work 2 times a week. Mix it with strength training. Activities like yoga or Tai Chi also help. They build flexibility and calm the mind.
Cognitive Exercises: Sharpening the Mind
Head injuries often hurt thinking skills. Cognitive exercises get the brain working again. They focus on memory, attention, and problem-solving. These tasks create new experiences to build neural connections.
One easy one is using your non-dominant hand. If you’re right-handed, brush your teeth with your left. This wakes up the other side of the brain. It strengthens cognitive function.
Brain-training apps are fun tools. Apps like Lumosity offer games and puzzles to improve memory. Play 15-20 minutes a day. They improve focus and speech.
Try memorization: Recall a grocery list. Start with 5 items, and add more. Or draw a map from memory. This builds usable memory.
Puzzles like Sudoku or crosswords challenge problem-solving. Jigsaws improve hand-eye coordination. Board games like chess enhance critical thinking and strategic planning skills.
Read out loud: Read a book or article aloud. It engages the reading, speaking, and listening parts of the brain.
Sensory exercises: Visit a market and identify the smells or tastes. This uses multiple senses to forge connections.
Start slow with simple tasks. Increase difficulty as you heal. Do them in a quiet place to avoid overload.
Chiropractic care helps with symptoms from head injuries. It eases headaches and dizziness. Chiropractors use adjustments to align the spine. This improves nervous system health and blood flow to the brain.
Craniosacral therapy is a gentle method. It uses a light touch on the head and spine. This boosts cerebrospinal fluid flow and reduces tension. It can help alleviate headaches and support neurological function.
Chiropractors often give lifestyle tips. They recommend healthy eating, adequate sleep, and regular exercise. This holistic approach speeds healing. Combining it with physical therapy can accelerate recovery.
Dr. Alexander Jimenez, a chiropractor with over 30 years of experience, observes that integrative care helps injury recovery. He uses functional medicine to address root causes. This includes nutrition and movement for better healing. His work demonstrates that chiropractic can effectively reduce pain without the need for drugs.
Techniques like neurofeedback and light therapy support brain healing. They promote neuroplasticity. Chiropractic neurology focuses on brain function following injuries.
Combining Exercises and Therapies: Tips for Success
Mix exercises for best results. Do aerobic, strength, balance, and cognitive work each week. Track progress in a journal. Take note of how you feel after each session.
Collaborate with a team of Doctors, therapists, and chiropractors. They can tailor a plan. Start at home with simple tools, such as water bottles or apps.
Rest is important. Sleep well and eat healthy foods. Avoid overdoing it to prevent setbacks.
Videos can guide you. One shows full-body strength workouts with squats and rows. Another has balance drills, such as cone reaching.
Consistency matters. Even small steps add up. With time, you’ll see improvements in movement, thinking, and balance.
Conclusion
Rehabilitation exercises are key to recovering from head injuries. They restore physical strength, cognitive sharpness, and balance. Combine aerobic walks, strength squats, balance exercises, and mental games. Add chiropractic care for symptom relief and nervous system support. Start slow, stay steady, and seek professional help. Recovery is possible with the right approach.
Healing from Within: How Traumatic Brain Injuries Create Body Toxicity and Integrative Care Supports Adult Recovery
Traumatic brain injuries, also known as TBIs, can abruptly alter a person’s life. For many adults, these injuries occur during a car crash on the way to work, a vicious hit in a weekend soccer game, or a fall at a construction site. These injuries do more than bruise the skull—they start a chain reaction of harm inside the body. This process creates a kind of “toxicity” that spreads from the brain to other organs, making recovery tough. But there’s hope. An integrative care approach, led by experts such as chiropractic nurse practitioners (CNPs), considers the whole person. It helps calm the body’s chaos, eases pain naturally, and builds strength for the long haul. Families and care teams also play a crucial role, providing emotional support and daily assistance. In this article, we’ll break down how TBIs cause this inner poison, why it matters for adults, and how team-based care can turn things around.
Imagine a 35-year-old office worker named Mark. He’s rear-ended in traffic, his head snaps back, and everything goes black for a moment. At first, it’s headaches and dizziness. Weeks later, gut issues and mood swings hit hard. The hidden side of TBI involves biochemical events that intensify over time. Research shows these effects can last weeks or years, raising risks for bigger problems like memory loss or even diseases like Alzheimer’s (Priester, 2025). But early, whole-body care changes the story. CNPs combine chiropractic adjustments with nursing expertise to reset the nervous system and combat inflammation. They guide adults like Mark back to work, play, and family life. This isn’t just medicine; it’s a roadmap for healing that honors the body’s own power.
For families, it’s personal. Spouses learn to spot warning signs, like when fatigue turns to frustration. Care teams coordinate visits, meals, and therapy sessions to ensure seamless care. Together, they tackle the toxicity head-on. As one study notes, addressing both the brain and body early can prevent long-term damage (Rauchman et al., 2023). Let’s dive into the science, simply explained, and see how recovery works in real life.
Understanding Traumatic Brain Injuries in Everyday Adult Life
Adults face TBIs more often than we think. In the U.S., over 2.8 million people seek emergency care each year, with motor vehicle accidents (MVAs) accounting for about 28%, falls at work for 20%, and sports-related injuries, such as those from football or boxing, making up another significant portion (Rauchman et al., 2023). A busy parent or factory worker can be out of work for months after a small slip or crash. Unlike children, adults often juggle jobs, bills, and family responsibilities, so recovery hits harder—lost wages, strained relationships, and endless doctor’s wait times.
A TBI starts with the primary injury: the direct hit. In an MVA, the brain slams against the skull, tearing blood vessels and nerves. Sports concussions come from rotational forces, twisting the brain like a wet towel. Workplace incidents, like dropping tools on the head, add blunt force. Right away, symptoms appear: confusion, nausea, and blurred vision. However, the real danger lies in the seconds that follow—the brain swells, pressure builds, and oxygen levels drop (Salehi et al., 2017).
Take Sarah, a 42-year-old soccer coach. A header in a pickup game leaves her with a mild concussion. She pushes through practices, but soon battles insomnia and irritability. Her family notices she’s “off.” This is common; mild TBIs affect 80% of cases, yet many adults ignore them, thinking it’s just a bump (Laskowitz & Grant, 2016). Men in their 30s and 40s, often in high-risk jobs or sports, make up the bulk. Women post-childbirth or in caregiving roles face extra stress, slowing healing.
Why does this matter? TBIs don’t stay in the head. They spark a body-wide alarm, releasing stress hormones that tax the heart and gut. Without quick care, simple tasks like driving become scary. But spotting it early helps. Doctors use CT scans for severe cases, but for mild ones, it’s a history and physical examination. Families step in here—tracking symptoms in a journal, urging rest. Workplaces can adapt with flexible hours or ergonomic fixes.
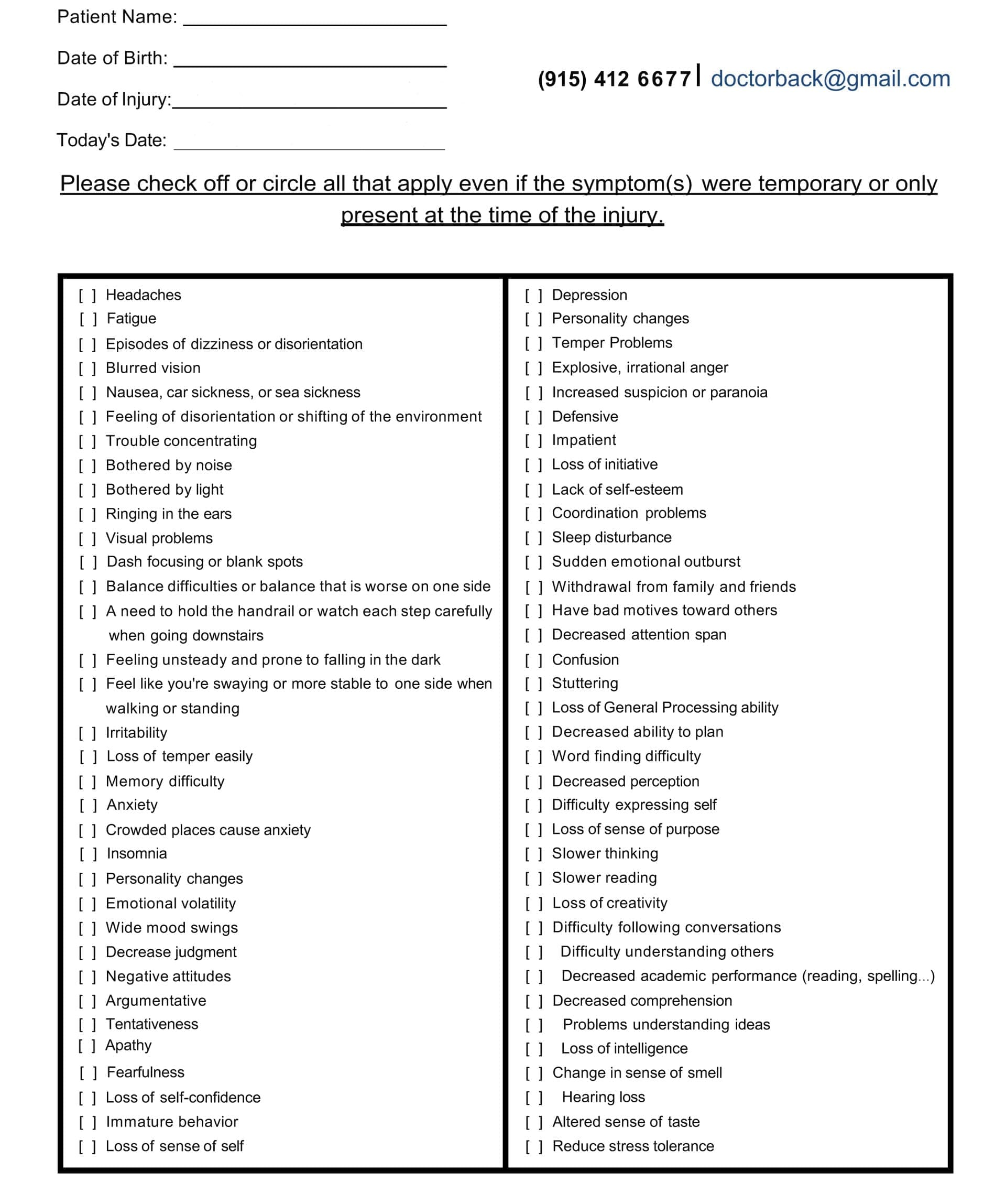
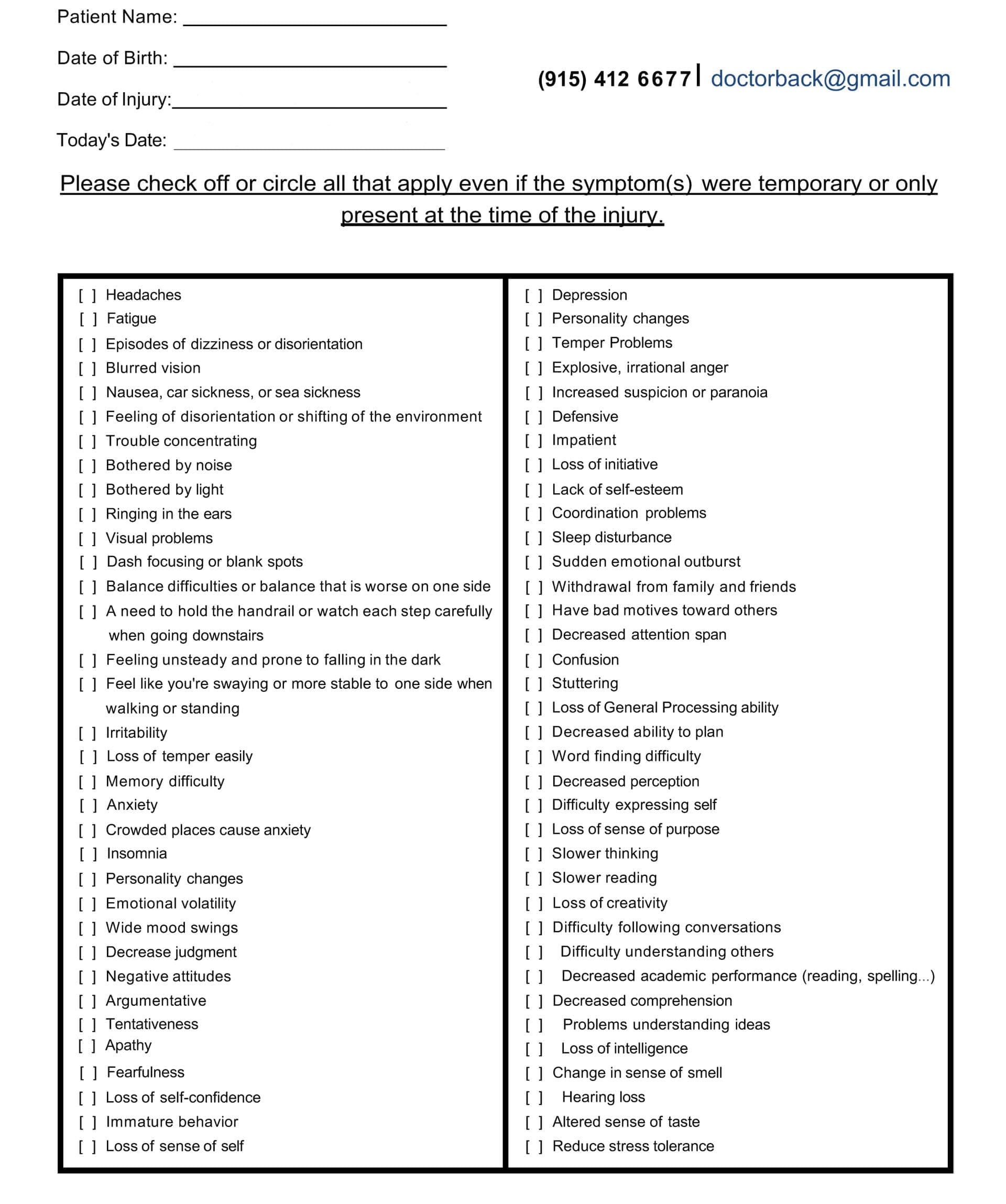
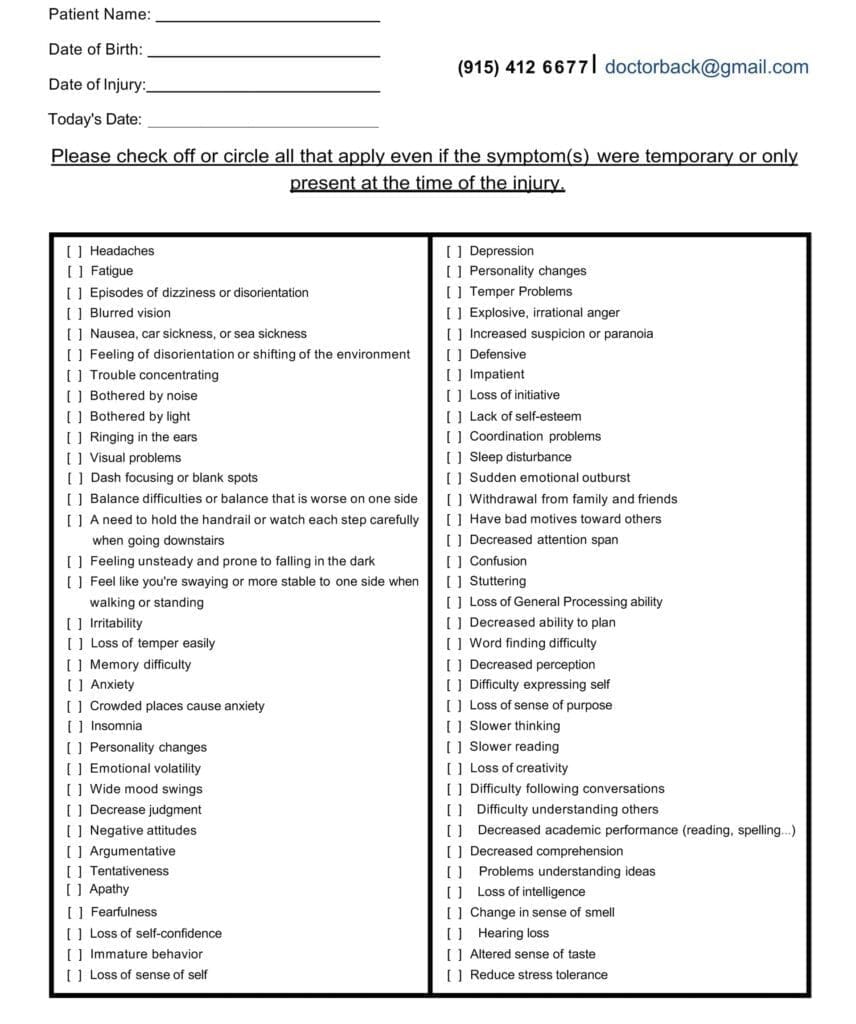
Symptom Questionnaire:
The positive news is that there are solutions available. Most adults recover well with support. One review found that 70% of patients return to normal within three months if treated holistically (Schimmel et al., 2017). That means blending rest, therapy, and family encouragement. For Mark from the intro, his wife joined therapy sessions, learning cues to de-escalate his frustration. It’s not just survival; it’s reclaiming life.
The Toxic Cascade: How TBIs Poison the Brain and Body
A TBI isn’t a one-and-done event. The initial impact, known as the primary injury, initiates a cascade of biochemical complications. This “cascade” turns the brain into a toxic zone, harming cells and spreading chaos to the gut, blood, and beyond. It’s like a fire that starts small but burns hot if unchecked. Understanding this helps adults and their teams fight back smarter.
Firstly, consider the initial impact. In an MVA, rapid deceleration shears axons—the brain’s wiring—like pulling threads from fabric. Sports-related impacts stretch tissue, while falling objects from work crush it. This releases danger signals, known as damage-associated molecular patterns (DAMPs), which alert the immune system (McKee & Lukens, 2016). Blood vessels break, starving cells of oxygen. Swelling, or edema, follows fast. There are two main types: cytotoxic, where cells suck up water like sponges due to pump failures, and vasogenic, where the blood-brain barrier (BBB) leaks like a busted dam, flooding tissue with proteins and fluid (Salehi et al., 2017). In adults, this raises skull pressure, squeezing the brain and risking more death. One study in mice showed edema peaking days after impact, mirroring human cases (Priester, 2025).
Now, the secondary storm—the real toxicity builder. It unfolds in phases: minutes, hours, days. Enter excitotoxicity. Damaged neurons release glutamate, the brain’s “go” signal, into the space. Normally, this excites cells briefly. However, in traumatic brain injury (TBI), it triggers a massive surge of glutamate. Glutamate overworks receptors, letting calcium rush in like floodwater. This calcium revs up destructive enzymes, which rip membranes and shred DNA. Cells swell, burst, and die in a chain reaction (Waters, n.d.). It’s why symptoms like seizures or coma are delayed. In car crashes, this “glutamate storm” spreads from impact zones, killing healthy neighbors (Rauchman et al., 2023). Adults in high-stress jobs often experience chronic fatigue, as their brains remain in overdrive.
Next, oxidative stress amps up the damage. The brain guzzles oxygen but has weak defenses. TBI sparks reactive oxygen species (ROS)—unstable molecules like superoxide or hydroxyl radicals—from busted mitochondria and fired-up immune cells. These ROS (reactive oxygen species) chew lipids in cell walls, creating toxic byproducts like 4-hydroxynonenal, which poison proteins and genes (Fesharaki-Zadeh, 2022). Iron from burst blood vessels fuels this process via Fenton reactions, generating more radicals. In sports concussions, repeated hits build ROS over time, explaining why pros face early Parkinson’s risks (Wu et al., 2022). One mouse study found that ROS stayed around for weeks after the infection, changing proteins and DNA in ways that are similar to the long-term symptoms of adults with persistent cognitive impairment (Priester, 2025).
Neuroinflammation piles on. Microglia, the brain’s guards, wake up and call in troops: monocytes via CCR2 signals and neutrophils, which release cytokines such as TNF-α and IL-1β (McKee & Lukens, 2016). This “fire” initially clears debris, but it then veers off course and attacks healthy tissue. In work injuries, chronic low-grade inflammation lingers, turning acute pain into a daily ache. Microglia also accumulate amyloid proteins, which serve as seeds for plaques in Alzheimer’s disease (Denniss & Barker, 2023). Cytokines breach the BBB, worsening leaks and edema. Adults report mood dips here—irritability from inflamed pathways mimicking depression.
Keep in mind the disruption of the gut-brain axis. The vagus nerve and microbes facilitate communication between the brain and gut. TBI shocks this link, slowing gut motility and poking holes in the intestinal wall—”leaky gut” (Faden et al., 2021). Bacteria enter the bloodstream, triggering sepsis or a body-wide inflammatory response. In MVAs, stress hormones like cortisol halt digestion, causing ulcers or symptoms similar to IBS (Heuer Fischer, P.A., n.d.). One study linked TBI-induced gut changes to worse brain swelling, as toxins circulate back via the blood (Cannon et al., 2023). For a construction worker, a post-fall condition means nausea on top of headaches, which can delay their return to the site.
These events interconnect: excitotoxicity generates ROS; inflammation widens the BBB cracks; gut leaks fuel the fire. The BBB, that tight shield of endothelial cells and astrocyte feet, frays from the action of matrix metalloproteinases (MMPs) and VEGF surges, allowing toxins to enter (Laskowitz & Grant, 2016a). Edema follows, compressing vessels and depriving cells of oxygen. In adults, this cascade hits harder—aging brains have less reserve, per one review (Salehi et al., 2017). However, is it possible to detect it at an early stage? Antioxidants, such as those in a new polymer, reduce ROS by 50% in mice, suggesting potential benefits in humans (Priester, 2025).
This toxicity isn’t abstract. For Sarah, the coach, it meant experiencing gut cramps and sidelining drills. Mark’s family adjusted meals to ease inflammation. Knowing the cascade empowers choice—enabling rest, consuming anti-inflammatory foods, and receiving targeted care. It’s the body’s cry for balance, and integrative pros listen.
Long-Term Risks: From Acute Toxicity to Lasting Brain Changes
If unchecked, TBI’s toxic wave doesn’t fade—it reshapes the brain. Weeks after the hit, waste like tau proteins piles up because the glymphatic system, the brain’s drain, clogs (Plog & Nedergaard, 2018). This mirrors the aging process or Alzheimer’s, where toxins spread, forming plaques. In adults, repeated sports hits can cause chronic traumatic encephalopathy (CTE)—mood swings, aggression, and dementia decades later (Priester, 2025).
Oxidative scars mutate genes; inflammation scars tissue with glial walls, blocking repair (Denniss & Barker, 2023). Gut leaks let endotoxins fuel chronic fatigue. One study tied early BBB breaks to poor outcomes years on (Laskowitz & Grant, 2016a). For work-hardened adults, this means early retirement and family strain. But mitigation works—lifestyle tweaks cut risks by 30% (Schimmel et al., 2017). It’s a wake-up: Act now, or pay later.
An Integrative Path to Recovery: The Role of Chiropractic Nurse Practitioners
Integrative care challenges the conventional understanding of TBI toxicity. It’s not just pills or scalpels—it’s a team that weaves chiropractic, nursing, nutrition, and therapy into one comprehensive plan. At the heart? Chiropractic nurse practitioners (CNPs). Trained in both fields, they identify spine-brain connections, adjust misalignments, and promote holistic healing. For adults post-MVA or concussion, this means less toxicity and more resilience.
Why chiropractic? The spine houses the nervous system; it conveys, constricts, and conveys signals. Adjustments realign the vertebrae, easing nerve pressure and resetting the “fight-or-flight” mode to a calm state (Sea Change Wellness Chiropractic, n.d.). One clinic notes it boosts cerebrospinal fluid (CSF) flow, the brain’s bath that clears toxins (Apex Chiropractic, n.d.). In workplace falls, this reduces headaches by 60%, according to patient reports (Northwest Florida Physicians Group, LLC, n.d.). CNPs add nursing layers by monitoring vitals, adjusting medications, and teaching self-care.
Dr. Alexander Jimenez, DC, APRN, FNP-BC, embodies this. At his El Paso clinic, he treats auto accident victims with spinal decompression and functional nutrition, targeting root causes like inflammation (Jimenez, n.d.a). “We restore normal functions after injuries without drugs,” he says, blending adjustments with omega-3s to douse ROS (Jimenez, n.d.b). His cases? A truck driver post-crash regained focus via neuropathy protocols; a golfer shook sports fog with vagus nerve stim via adjustments. Over 30 years, he’s seen integrative plans slash recovery time, empowering adults to ditch painkillers.
This approach hits all cascades. For excitotoxicity, gentle cranial work calms glutamate storms (Dr. Kal, n.d.). Oxidative stress? CNPs promote the uptake of antioxidants—such as berries and vitamin E—to neutralize ROS, a finding supported by mouse studies (Wu et al., 2022). Neuroinflammation can be alleviated with posture adjustments, thereby reducing cytokine triggers (Serenity Healthcare Partners, n.d.). Gut-brain? Probiotics and vagus-focused breathing mend leaks (Faden et al., 2021). BBB heals via better circulation from alignments.
Integrated therapies shine. Physical therapy helps rebuild balance, while CBT tames anxiety (Peixoto et al., 2025). Nutrition—anti-inflammatory diets—fuels repair (Serenity Healthcare Partners, n.d.). Emerging technologies, such as EMF stimulation in swine models, restore brain waves, hinting at potential human applications (Brazdzionis et al., 2023). CNPs coordinate, personalizing for a 50-year-old welder’s shifts or a mom’s school runs.
For Mark, CNP-led sessions mixed adjustments with family nutrition classes. Sarah added yoga for gut calm. Results? Sarah experienced faster clarity and fewer trips to the emergency room. Dr. Jimenez’s webinars stress this: “Functional medicine reverses imbalances—oxidative stress, gut dysbiosis—for true recovery” (Jimenez, n.d.b). It’s empowering, natural, and effective.
Supporting the Journey: Families and Care Teams in Adult TBI Recovery
Recovery isn’t solo. Families and care teams are the glue, turning plans into action. Spouses track moods, spotting toxicity flares like irritability from inflammation. Kids adapt games for dad’s fatigue; siblings share chores. This buffer cuts depression risks by 40% (Peixoto et al., 2025).
Care teams—CNPs, therapists, and docs—huddle weekly, adjusting for work stress or sports urges. Families attend education sessions to learn about edema signs or gut-friendly meal options. One family’s story: Post-concussion, they mapped “rest zones” at home, easing Mark’s load. Emotional tools, such as support groups, build resilience. As Dr. Jimenez notes, “Holistic care includes mind and spirit—families amplify healing” (Jimenez, n.d.a). It’s a shared victory.
Conclusion: Reclaiming Life After the Storm
TBIs from crashes, games, or jobs unleash a toxic cascade—excitotoxicity flooding cells, ROS scorching tissues, inflammation raging, and gut links breaking. For adults, it’s a body-wide battle, but integrative care, spearheaded by CNPs, counters it. Adjustments reset nerves, nutrition quells fires, and teams sustain hope. With families involved, recovery isn’t just possible—it’s transformative. As research evolves, from antioxidants to EMF, the path brightens. Adults like Mark and Sarah prove: Healing starts within but thrives together. Seek care early; your future self will thank you.
Brazdzionis, J., Radwan, M. M., Thankam, F., Lal, M. R., Baron, D., Connett, D. A., Agrawal, D. K., & Miulli, D. E. (2023). A swine model of traumatic brain injury: Effects of neuronally generated electromagnetic fields and electromagnetic field stimulation on traumatic brain injury-related changes. Cureus, 15(11), e48992. https://doi.org/10.7759/cureus.48992
Cannon, A. R., Anderson, L. J., Galicia, K., Murray, M. G., Kamran, A. S., Li, X., Gonzalez, R. P., & Choudhry, M. A. (2023). Traumatic brain injury induced inflammation and GI motility dysfunction. Brain Sciences, 13(3), 414. https://doi.org/10.3390/brainsci13030414
Denniss, R. J., & Barker, L. A. (2023). Brain trauma and the secondary cascade in humans: Review of the potential role of vitamins in reparative processes and functional outcome. Neuropsychiatric Disease and Treatment, 19, 1693–1707. https://doi.org/10.2147/NDT.S415943
Faden, A. I., Barrett, J. P., Stoica, B. A., & Henry, R. J. (2021). Bi-directional brain-systemic interactions and outcomes after TBI. Trends in Neurosciences, 44(5), 406–418. https://doi.org/10.1016/j.tins.2020.12.004
Fesharaki-Zadeh, A. (2022). Oxidative stress in traumatic brain injury. International Journal of Molecular Sciences, 23(21), 13000. https://doi.org/10.3390/ijms232113000
Laskowitz, D., & Grant, G. (Eds.). (2016a). Blood–brain barrier pathophysiology following traumatic brain injury. In Translational research in traumatic brain injury. CRC Press/Taylor & Francis Group. https://www.ncbi.nlm.nih.gov/books/NBK326726/
Laskowitz, D., & Grant, G. (Eds.). (2016b). Neuroplasticity after traumatic brain injury. In Translational research in traumatic brain injury. CRC Press/Taylor & Francis Group. https://www.ncbi.nlm.nih.gov/books/NBK326735/
McKee, C. A., & Lukens, J. R. (2016). Emerging roles for the immune system in traumatic brain injury. Frontiers in Immunology, 7, 556. https://doi.org/10.3389/fimmu.2016.00556
Peixoto, B., Cruz, M., & Ustares, V. (2025). Traumatic brain injury and neuropsychiatric consequences. Current Psychiatry Reports, 27(1), 1–12. https://doi.org/10.1007/s11920-024-01523-4
Plog, B. A., & Nedergaard, M. (2018). The glymphatic system in CNS health and disease. Neuron, 98(6), 1095–1118. (From rehabpub.com summary)
Rauchman, S. H., Zubair, A., Jacob, B., Rauchman, D., Pinkhasov, A., & Placantonakis, D. G. (2023). Traumatic brain injury: Mechanisms, manifestations, and visual sequelae. Frontiers in Neuroscience, 17, 1090672. https://doi.org/10.3389/fnins.2023.1090672
Salehi, A., Zhang, J. H., & Obenaus, A. (2017). Response of the cerebral vasculature following traumatic brain injury. Journal of Cerebral Blood Flow & Metabolism, 37(10), 2320–2339. https://doi.org/10.1177/0271678X17701660
Schimmel, S. J., Acosta, S., & Lozano, D. (2017). Neuroinflammation in traumatic brain injury: A chronic response to an acute injury. Journal of Neurotrauma, 34(13), 2139–2147. https://doi.org/10.1089/neu.2016.4648
Learn how cognitive impairment relates to traumatic brain injury. Discover symptoms, diagnosis, and recovery strategies.
Introduction
One of the biggest health problems of our time is brain damage, which affects millions of individuals every year and has effects that endure long after the original injury. Over 30% of injury-related fatalities in the US include some kind of brain trauma, making traumatic brain injuries a leading cause of mortality and disability globally (Bailes & Borlongan, 2020). These wounds set off an intricate series of events that alter not only how the brain works but also how the body as a whole functions. missionlegalcenter Two separate stages of damage occur when a person gets a traumatic brain injury. The main harm occurs when external forces instantly induce mechanical damage to brain tissue at the point of contact. A secondary damage phase follows, when biochemical processes such as oxidative stress, inflammation, cell death, and other detrimental alterations cause the brain to gradually deteriorate over the course of days, weeks, and even months after the original trauma (Bailes & Borlongan, 2020). Healthcare professionals may create more effective treatment plans that address both short-term issues and long-term healing requirements by having a better understanding of these injury patterns. missionlegalcenter Cognitive impairment represents one of the most common and challenging consequences of traumatic brain injury. Problems with attention, memory, and executive functioning emerge as the primary neurocognitive consequences across all levels of injury severity (Cognitive Impairment Following Traumatic Brain Injury, 2002). These cognitive disruptions profoundly affect daily life, making it difficult for individuals to work, maintain relationships, manage household tasks, and participate fully in their communities. Because attention and memory serve as foundational cognitive abilities, their disruption can trigger additional problems with executive function, communication, and other complex mental processes (Cognitive Impairment Following Traumatic Brain Injury, 2002).pubmed.ncbi.nlm.nih
The connection between brain and body becomes especially important when considering traumatic brain injury recovery. The brain controls virtually every function in the human body through an intricate network of nerves and chemical signals. The central nervous system, comprising the brain and spinal cord, regulates awareness, movement, sensation, thought, speech, and memory (Anatomy and physiology of the nervous system, 2020). When injury disrupts these control centers, the effects ripple throughout the entire body, affecting muscles, bones, organs, and metabolic processes.cancer An integrative approach that combines chiropractic care with nurse practitioner oversight offers promising possibilities for individuals recovering from traumatic brain injuries. This collaborative model addresses the neurological, musculoskeletal, cognitive, emotional, and metabolic aspects of recovery. Chiropractic care focuses on restoring nervous system function through spinal adjustments, soft-tissue therapies, and targeted exercises, while nurse practitioners provide comprehensive medical management, cognitive support, and coordination of overall health needs. Together, these providers can create comprehensive treatment plans that support the brain’s natural healing processes and help patients regain function and improve their quality of life.
What is a Traumatic Brain Injury?
Traumatic brain injury refers to brain damage caused by an outside force that disrupts normal brain function. This external force can take many forms, including a forceful bump, blow, or jolt to the head or body, or an object penetrating the skull and damaging brain tissue (Traumatic Brain Injury, 2023). The injury occurs when the brain moves violently inside the skull or when an external object breaks through the skull barrier. Common causes include motor vehicle accidents, falls, sports injuries, violence, and blast exposures from explosions (Types of Traumatic Brain Injury, 2024).ninds.nih+1 Healthcare providers classify traumatic brain injuries according to their severity, which helps guide treatment decisions and predict outcomes. The three main categories include mild, moderate, and severe traumatic brain injury. Medical professionals use several measures to determine severity, including the Glasgow Coma Scale score, duration of loss of consciousness, length of post-traumatic amnesia, and results from brain imaging studies (Criteria used to classify TBI severity, 2012).ncbi.nlm.nih+1
Mild traumatic brain injury, often called a concussion, generally does not cause prolonged loss of consciousness. If unconsciousness occurs, it typically lasts less than thirty minutes. The Glasgow Coma Scale score ranges from thirteen to fifteen for mild injuries. Common symptoms include headaches, dizziness, confusion, nausea, vision problems, difficulty thinking clearly, balance issues, sleep disturbances, sensitivity to light and sound, problems with attention and concentration, fatigue, anxiety, irritability, and emotional changes (4 Types of Brain Injuries and 3 Levels of Severity, 2021). Memory loss associated with mild traumatic brain injury usually lasts less than twenty-four hours. Most people with mild injuries recover within a few days to weeks with appropriate rest and management (4 Types of Brain Injuries and 3 Levels of Severity, 2021).missionlegalcenter
Moderate traumatic brain injury involves unconsciousness lasting more than thirty minutes but less than twenty-four hours. The Glasgow Coma Scale score falls between nine and twelve. Individuals with moderate injuries experience all the symptoms associated with mild traumatic brain injury, plus additional concerning signs. These include headaches that worsen or do not improve, seizures or convulsions, numbness or weakness in the arms and legs, repeated vomiting, inability to wake from sleep, and slurred speech (4 Types of Brain Injuries and 3 Levels of Severity, 2021). Post-traumatic amnesia lasts more than one day but less than seven days. Brain imaging may show abnormalities such as bleeding, bruising, or swelling (Criteria used to classify TBI severity, 2012).ncbi.nlm.nih+1
Severe traumatic brain injury represents the most serious category, with loss of consciousness exceeding twenty-four hours. The Glasgow Coma Scale score ranges from three to eight. Post-traumatic amnesia persists for more than seven days. Individuals with severe injuries often require intensive medical care and extended rehabilitation. They may experience altered consciousness states, including coma, vegetative state, or minimally conscious state (Traumatic Brain Injury, 2023). Brain imaging typically reveals significant abnormalities including bleeding within the brain tissue, bleeding over the brain surface, bleeding in the brain’s ventricles, swelling, and tissue damage (Types of Traumatic Brain Injury, 2024).medschool.ucla+1
The type of traumatic brain injury also provides important classification information. Closed head injuries occur when the head experiences impact or rapid movement without skull penetration. Concussions, diffuse axonal injury, and contusions fall into this category. Diffuse axonal injury, one of the most common types, involves widespread damage to the brain’s white matter, which contains nerve fibers that facilitate communication between different brain regions. This type of injury commonly happens in auto accidents, falls, and sports-related trauma (Traumatic Brain Injury, 2023). Penetrating brain injuries occur when an object breaks through the skull and enters brain tissue, as seen with gunshot wounds or impalement injuries (Types of Traumatic Brain Injury, 2024).ninds.nih+1 Understanding whether an injury is primary or secondary helps guide treatment approaches. Primary traumatic brain injury refers to the immediate structural damage inside the brain resulting directly from the initial impact. This includes bruising, bleeding, and tearing of brain tissue and blood vessels. Secondary traumatic brain injury describes complications that develop after the initial trauma and cause additional damage to an already compromised brain. Secondary injury mechanisms include increased pressure inside the skull, progressive brain swelling, damage to blood vessels triggering stroke or seizures, and lack of oxygen related to blood pressure drops or breathing difficulties (Types of Traumatic Brain Injury, 2024).medschool.ucla
How TBI Causes Cognitive Impairment
Traumatic brain injury triggers a complex series of events that disrupt normal brain function and lead to cognitive impairment. Understanding these mechanisms enables healthcare providers to develop targeted interventions that support recovery and effectively manage symptoms.
The physical damage from traumatic brain injury affects brain structure and function in multiple ways. When the brain experiences trauma, nerve cells can be stretched, torn, or destroyed. The white matter tracts that connect different brain regions become damaged, disrupting the communication networks essential for coordinated brain function. Diffuse axonal injury particularly affects these communication pathways, as the nerve fibers that transmit signals between brain cells break down and lose their ability to conduct information efficiently (Traumatic Brain Injury, 2023).ninds.nih
Bleeding within the brain creates additional problems. When blood vessels rupture, blood accumulates in spaces where it does not belong, creating pressure that compresses surrounding brain tissue. This compression damages cells both directly through physical pressure and indirectly by reducing blood flow to affected areas. Swelling further compounds these problems, as increased fluid within the rigid skull creates mounting pressure that can damage brain tissue and reduce oxygen delivery (Types of Traumatic Brain Injury, 2024).medschool.ucla
At the cellular level, traumatic brain injury initiates harmful biochemical cascades. Cell membranes become disrupted, allowing excessive calcium and sodium to enter neurons. This triggers a series of destructive processes including activation of enzymes that break down cellular components, production of free radicals that damage cell structures, mitochondrial dysfunction that impairs energy production, and release of inflammatory molecules that promote further injury (Bailes & Borlongan, 2020). These processes can continue for days, weeks, or even months after the initial injury, explaining why symptoms sometimes worsen or new problems emerge well after the traumatic event.missionlegalcenter
Inflammation plays a particularly important role in post-traumatic brain injury cognitive impairment. Within seconds after trauma, inflammatory responses activate in the brain. The blood-brain barrier, which normally protects the brain from harmful substances in the bloodstream, becomes damaged and allows inflammatory cells and molecules to enter brain tissue. While some inflammation helps with healing and clearing damaged tissue, excessive or prolonged inflammation damages healthy brain cells and interferes with recovery. Inflammatory molecules affect neurotransmitter systems, disrupt nerve signaling, and impair the formation of new neural connections needed for cognitive recovery (Mesenchymal stem cell therapy alleviates the neuroinflammation, 2020).medicine.washu
Different brain regions show varying vulnerability to traumatic injury, which explains the specific cognitive impairments that develop. The frontal lobes, responsible for executive functions such as planning, decision-making, impulse control, and working memory, are particularly susceptible to damage from trauma. The temporal lobes, involved in memory formation and language processing, also commonly sustain injury. Damage to the hippocampus, a structure critical for forming new memories, explains why memory problems rank among the most frequent cognitive complaints after traumatic brain injury (Cognitive Problems After Traumatic Brain Injury, n.d.).uwmsktc.washington
Attention and concentration problems emerge as foundational deficits following traumatic brain injury. Individuals may struggle to focus, pay attention to relevant information while filtering out distractions, or attend to more than one task at a time. This leads to restlessness, easy distractibility, difficulty finishing projects, problems carrying on conversations, and trouble sitting still for extended periods. Because attention skills serve as building blocks for higher-level cognitive abilities, people with attention problems often develop additional difficulties with memory, reasoning, and problem-solving (Cognitive Problems After Traumatic Brain Injury, n.d.).uwmsktc.washington
Processing speed commonly slows after brain injury. Individuals take longer to understand what others are saying, need more time to follow directions, struggle to keep up with television shows or movies, require additional time to read and comprehend written material, and show delayed reactions to stimuli. This slowed processing affects everyday activities and can make tasks that were once automatic feel laborious and exhausting. The reduced reaction time poses particular concerns for activities requiring quick responses, such as driving (Cognitive Problems After Traumatic Brain Injury, n.d.).uwmsktc.washington
Memory impairments manifest in various ways after traumatic brain injury. Short-term memory problems make it difficult to hold information in mind temporarily, such as remembering a phone number long enough to dial it or recalling items on a shopping list. Long-term memory difficulties affect the ability to store and retrieve information over extended periods. People may struggle to remember recent events, learn new information, or recall facts and procedures they previously knew well. Working memory, which involves holding and manipulating information simultaneously, becomes compromised, affecting complex cognitive tasks like mental arithmetic, following multi-step directions, and reasoning (Cognitive Impairment Following Traumatic Brain Injury, 2002).pubmed.ncbi.nlm.nih
Executive function deficits represent another hallmark of traumatic brain injury cognitive impairment. Executive functions include the mental processes that help people plan activities, organize information, initiate tasks, monitor performance, shift between tasks flexibly, solve problems, make decisions, and control impulses. When these abilities become impaired, individuals struggle with goal-directed behavior, adapting to new situations, regulating emotions, and functioning independently in daily life (Cognitive Problems After Traumatic Brain Injury, n.d.).uwmsktc.washington
The Brain-Body Connection
The relationship between the brain and body represents one of the most fundamental aspects of human physiology. This intricate connection enables all body functions, from voluntary movements to unconscious processes that sustain life. Understanding this connection becomes especially important when considering how traumatic brain injury affects not just cognitive abilities but overall physical health and function.
The central nervous system serves as the command center for the entire body. Made up of the brain and spinal cord, this system controls awareness, movements, sensations, thoughts, speech, and the five senses of seeing, hearing, feeling, tasting, and smelling (Central nervous system function, 2025). The brain manages most body functions by processing information from sensory receptors throughout the body and sending out instructions through an extensive network of nerves. The spinal cord acts as an extension of the brain, carrying messages between the brain and peripheral nerves that reach every part of the body (Central nervous system function, 2025).healthdirect
The peripheral nervous system complements the central nervous system by connecting the brain and spinal cord to the rest of the body. This network of nerves and ganglia sends signals to and receives signals from the central nervous system, enabling two-way communication between the brain and body tissues. The peripheral nervous system divides into the somatic nervous system, which controls voluntary movements like walking and grasping objects, and the autonomic nervous system, which manages involuntary functions that the body performs automatically, such as breathing, heartbeat, digestion, and blood pressure regulation (Anatomy and physiology of the nervous system, 2020).cancer
The autonomic nervous system further separates into two complementary branches that maintain balance in body functions. The sympathetic nervous system prepares the body for situations requiring strength, heightened awareness, or rapid response, commonly known as the fight-or-flight response. Activation of this system increases heart rate, elevates blood pressure, speeds breathing, dilates pupils, and increases metabolic rate. The parasympathetic nervous system creates opposite effects, returning heart rate and breathing to normal, constricting pupils, and slowing metabolism to conserve energy and promote rest and recovery (Anatomy and physiology of the nervous system, 2020).cancer
Research demonstrates that the brain and body maintain constant, bidirectional communication through multiple pathways. Recent studies show that parts of the brain area controlling movement connect directly to networks involved in thinking, planning, and control of involuntary body functions such as blood pressure and heartbeat. This literal linkage of body and mind in brain structure helps explain phenomena like why anxiety makes people pace, why vagus nerve stimulation can alleviate depression, and why regular exercise improves mental outlook (Mind-body connection is built into brain, 2023).medicine.washu
The vagus nerve exemplifies this brain-body connection. This cranial nerve carries signals between the brain and internal organs, providing information about organ function and regulating processes like digestion and heart rate. Signals traveling through the vagus nerve are coded independently by specialized neurons, allowing the brain to discriminate precisely among various body signals and respond appropriately. This sophisticated communication system enables the brain to monitor and adjust organ function continuously based on changing body needs and environmental demands (Revealing Communications Between Brain and Body, 2022).medicine.yale
Blood flow represents another critical aspect of brain-body connection. The brain, despite constituting only about two percent of total body mass, consumes over twenty percent of the body’s glucose-derived energy. Continuous glucose metabolism supports neuronal signaling, as adenosine triphosphate, the cell’s energy currency, powers action potentials, maintains ionic gradients, and supports synaptic transmission. Because the brain cannot synthesize or store glucose independently, it depends entirely on glucose from dietary intake and blood circulation. Any disruption to blood flow or energy metabolism can significantly impair brain function (Metabolic hormones mediate cognition, 2009).sciencedirect
The musculoskeletal system connects intimately with brain function through sensory feedback and motor control. Muscles contain specialized receptors that constantly send information to the brain about body position, movement, and force. This proprioceptive feedback allows the brain to coordinate movement, maintain posture, and adjust to environmental demands. The brain processes this information and sends motor commands back to muscles, enabling precise, coordinated movement. When traumatic brain injury disrupts these communication pathways, both sensory perception and motor control become impaired (Nervous System Function, 2024).clevelandclinic
Hormonal systems provide another dimension of brain-body connection. The hypothalamus and pituitary gland, located deep within the brain, regulate hormonal signals that control growth, metabolism, reproduction, stress response, and many other functions. These structures form a feedback loop, with the hypothalamus releasing hormones that signal the pituitary gland, which then distributes hormones to various body systems including the adrenal glands, thyroid, reproductive organs, skin, bone, and muscle. This hormonal regulation affects mood, memory, metabolism, muscle mass, energy levels, stress response, and reproductive function (Neuroendocrine Disturbances Following TBI, 2023).biausa
The immune system also maintains constant communication with the brain. Immune cells and inflammatory molecules can cross from the bloodstream into brain tissue, particularly when the blood-brain barrier becomes damaged following injury. The brain, in turn, can influence immune function through neural and hormonal signals. This bidirectional communication becomes particularly important following traumatic brain injury, when both local brain inflammation and systemic immune responses affect recovery and long-term outcomes (Multiorgan Dysfunction After Severe TBI, 2021).pmc.ncbi.nlm.nih
Causes and Symptoms of Cognitive Impairment
Cognitive impairment following traumatic brain injury arises from multiple interrelated causes that affect brain structure and function. Understanding these causes enables healthcare providers to identify risk factors, develop effective prevention strategies, and tailor targeted treatment approaches.
The primary cause of cognitive impairment stems from direct damage to brain tissue at the moment of injury. When the brain experiences sudden acceleration, deceleration, or rotational forces, nerve cells stretch and tear, blood vessels rupture, and tissue bruises. The specific location and extent of damage determine which cognitive functions become impaired. Injuries to the frontal lobes typically affect executive functions, attention, and working memory. Damage to the temporal lobe disrupts memory formation and language processing. Parietal lobe injuries interfere with sensory processing and spatial awareness, while occipital lobe damage affects visual processing (Traumatic Brain Injury, 2023).ninds.nih
Secondary injury mechanisms compound the initial damage. Swelling increases pressure within the rigid skull, compressing brain tissue and reducing blood flow. Bleeding creates masses that displace normal brain structures and increase intracranial pressure. Chemical imbalances develop as damaged cells release excessive amounts of neurotransmitters, particularly glutamate, which overstimulates neighboring neurons and triggers cell death. Free radicals produced during cellular metabolism damage cell membranes and DNA. Mitochondrial dysfunction impairs energy production, leaving neurons unable to maintain normal function. These secondary processes continue for days to weeks after the initial injury, explaining why cognitive symptoms may worsen or emerge gradually (Bailes & Borlongan, 2020).missionlegalcenter
Inflammation represents a major contributor to cognitive impairment following traumatic brain injury. The inflammatory response activates within seconds after trauma and can persist for months or even years. While acute inflammation helps remove damaged tissue and initiate healing, chronic inflammation damages healthy neurons and interferes with recovery. Inflammatory molecules disrupt neurotransmitter systems, impair synaptic plasticity, reduce the production of growth factors needed for neural repair, and contribute to the ongoing death of brain cells. This persistent inflammation particularly affects cognitive functions requiring complex neural networks and plasticity, such as learning, memory consolidation, and executive function (Mesenchymal stem cell therapy alleviates the neuroinflammation, 2020).medicine.washu
Disrupted blood flow contributes to cognitive impairment by reducing oxygen and nutrient delivery to brain tissue. Traumatic brain injury can damage blood vessels directly, alter blood pressure regulation, and trigger vasospasm where blood vessels constrict excessively. The brain requires constant, abundant blood supply to meet its high metabolic demands. Even brief or partial reductions in blood flow can impair neural function and contribute to cell death. Chronic reductions in cerebral blood flow may explain some persistent cognitive deficits that remain long after the initial injury (Long-term Consequences of TBI in Bone, 2018).pmc.ncbi.nlm.nih
Hormonal disruptions following traumatic brain injury affect cognition through multiple pathways. The hypothalamus and pituitary gland, structures that regulate hormonal systems, are particularly vulnerable to traumatic injury due to their location and delicate structure. Damage to these areas causes hypopituitarism, a condition where insufficient hormone production affects growth, metabolism, stress response, and reproduction. Growth hormone deficiency, thyroid hormone deficiency, and sex hormone deficiencies all contribute to cognitive impairment, affecting memory, attention, processing speed, and executive function (Neuroendocrine Disturbances Following TBI, 2023).biausa
The symptoms of cognitive impairment following traumatic brain injury vary widely depending on injury severity, location, and individual factors. Attention and concentration problems rank among the most common complaints. Individuals struggle to focus on tasks, become easily distracted by environmental stimuli, have difficulty filtering out irrelevant information, and cannot maintain attention for extended periods. These problems make it challenging to follow conversations, complete work tasks, read for comprehension, or perform activities requiring sustained mental effort (Cognitive Problems After Traumatic Brain Injury, n.d.).uwmsktc.washington
Memory impairments manifest in various ways. Short-term memory problems make it difficult to remember recent events, conversations, or instructions. People may repeatedly ask the same questions, forget appointments, or lose track of items. Long-term memory difficulties affect the ability to recall past events, previously learned information, or familiar procedures. Working memory deficits interfere with tasks requiring simultaneous information holding and manipulation, such as mental calculations, following multi-step directions, or reasoning through problems (Cognitive Impairment Following Traumatic Brain Injury, 2002).pubmed.ncbi.nlm.nih
Processing speed reductions cause delays in understanding and responding to information. Individuals take longer to comprehend spoken or written language, need extra time to formulate responses, show slowed reaction times, and struggle to keep pace in conversations or fast-moving situations. This slowed processing affects virtually all cognitive tasks and creates frustration when individuals recognize their difficulties but cannot overcome them through effort alone (Cognitive Problems After Traumatic Brain Injury, n.d.).uwmsktc.washington
Executive function deficits create problems with higher-order cognitive processes. People struggle with planning and organizing activities, initiating tasks without prompting, maintaining focus on long-term goals, shifting flexibly between tasks or mental sets, monitoring their own performance, solving novel problems, making sound decisions, and controlling impulses. These difficulties severely impact independence, as they interfere with managing finances, maintaining employment, keeping appointments, completing household tasks, and regulating behavior in social situations (Cognitive Problems After Traumatic Brain Injury, n.d.).uwmsktc.washington
Communication problems often accompany cognitive impairment. Individuals may have difficulty finding the right words, organizing their thoughts coherently, following complex conversations, understanding nonliteral language like sarcasm or idioms, interpreting social cues, or maintaining appropriate topics in conversation. These challenges affect relationships and social participation, contributing to isolation and reduced quality of life (Cognitive Impairment Following Traumatic Brain Injury, 2002).pubmed.ncbi.nlm.nih
Learning difficulties emerge when cognitive impairment affects the ability to acquire new information or skills. People need more repetition to learn new material, struggle to transfer learned skills to new situations, have difficulty recognizing patterns, and cannot efficiently organize information for storage and retrieval. These learning problems affect vocational rehabilitation, academic pursuits, and adaptation to life changes necessitated by the injury (Cognitive Impairment Following Traumatic Brain Injury, 2002).pubmed.ncbi.nlm.nih
Effects on Musculoskeletal and Neurological Systems
Traumatic brain injury creates widespread effects throughout the musculoskeletal and neurological systems, affecting movement, coordination, sensation, and physical integrity. These effects arise from both direct injury to neural structures that control these systems and secondary changes that develop over time. The musculoskeletal system experiences significant impacts following traumatic brain injury through multiple mechanisms. Spasticity, characterized by increased muscle tone and involuntary muscle contractions, develops in a substantial proportion of individuals with moderate to severe traumatic brain injury. The degree of spasticity varies from mild muscle stiffness to severe, painful, uncontrollable muscle spasms. Affected muscles may resist passive stretching, contract involuntarily, and develop shortened resting length over time. Spasticity interferes with movement, positioning, comfort, and functional activities. It can lead to joint contractures, pain, skin breakdown, and difficulty with daily care (TBI-Induced Spasticity, 2015).ncbi.nlm.nih
Muscle weakness and paralysis occur when traumatic brain injury damages motor cortex areas or descending motor pathways that transmit movement commands from brain to muscles. The pattern and severity of weakness depend on injury location. Hemiparesis, weakness affecting one side of the body, develops when injury occurs to motor areas in one brain hemisphere. Quadriparesis involves weakness in all four limbs. Even mild weakness significantly impacts function, affecting walking, reaching, grasping, and other essential movements. Muscle atrophy, or wasting, develops over time when muscles cannot be used normally due to weakness or inactivity (Physical effects of brain injury, n.d.).headway
Balance and coordination problems represent common musculoskeletal consequences of traumatic brain injury. Damage to the cerebellum, a brain structure that coordinates movement, causes ataxia characterized by unsteady gait, difficulty with fine motor tasks, tremor during purposeful movements, and impaired ability to judge distances. Balance problems also arise from vestibular system damage, proprioceptive deficits, visual processing impairments, and motor control difficulties. These balance and coordination deficits increase fall risk, limit mobility, and reduce independence in daily activities (Physical effects of brain injury, n.d.).headway
Post-traumatic seizures develop in some individuals following traumatic brain injury, representing neurological system dysfunction. Seizures can occur immediately after injury, within the first week, or months to years later. They result from abnormal electrical activity in damaged brain tissue. The risk increases with injury severity, presence of bleeding in the brain, skull fractures, and penetrating injuries. Seizures interfere with daily activities, increase injury risk, and may worsen cognitive impairment if not well controlled (Traumatic Brain Injury, 2023).ninds.nih
Sensory disturbances commonly accompany traumatic brain injury. Individuals may experience numbness, tingling, burning sensations, or altered temperature perception. Pain syndromes develop, including headaches, neck pain, and widespread body pain. These sensory changes result from damage to sensory processing areas in the brain, peripheral nerves, or spinal structures often injured concurrently with traumatic brain injury. Chronic pain significantly affects quality of life, mood, sleep, and rehabilitation participation (Pain and Traumatic Brain Injury, 2024).health
Vestibular dysfunction affects up to fifty percent of traumatic brain injury patients at five years post-injury. The vestibular system, which controls balance and spatial orientation, can be damaged at the peripheral level in the inner ear, at the central level in the brain, or both. Common vestibular diagnoses following traumatic brain injury include benign paroxysmal positional vertigo, where calcium crystals in the inner ear become displaced causing brief spinning sensations with position changes; acute unilateral peripheral vestibular loss, where one inner ear loses function; and migraine-associated vertigo. Vestibular dysfunction causes dizziness, vertigo, imbalance, nausea, and difficulty with activities requiring head movement. Interestingly, many individuals with objective vestibular dysfunction do not report symptoms, likely because traumatic brain injury affects perceptual mechanisms (Vestibular dysfunction in acute TBI, 2019).pmc.ncbi.nlm.nih
Vision and eye movement problems affect up to ninety percent of traumatic brain injury patients. These problems include difficulty tracking moving objects smoothly, impaired ability to shift gaze rapidly between targets, reduced convergence ability needed for near vision tasks, double vision from misalignment of the eyes, difficulty focusing, reduced visual field, and light sensitivity. These visual disturbances result from damage to cranial nerves that control eye muscles, brain areas that process visual information, or brain regions that coordinate eye movements. Visual dysfunction significantly impacts reading, driving, balance, and participation in rehabilitation activities (Eye Movement Problems After Brain Injury, 2021).optometrists+1
The skeletal system experiences long-term consequences from traumatic brain injury that are less obvious but clinically significant. Research shows that traumatic brain injury patients have increased risk of osteopenia and osteoporosis, conditions characterized by reduced bone mineral density and increased fracture risk. Bone loss occurs through multiple mechanisms, including reduced physical activity, hormonal disruptions affecting bone metabolism, vitamin D deficiency, inflammation, and altered bone formation and resorption signaling. Adults with traumatic brain injury show accelerated bone mineral density loss in the femur, particularly within the first year after injury. This increased skeletal fragility raises concern for future fractures that could complicate recovery and independence (Long-term Consequences of TBI in Bone, 2018).pmc.ncbi.nlm.nih
Heterotopic ossification, the formation of bone in soft tissues where bone should not normally exist, develops in some traumatic brain injury patients. This condition commonly affects muscles and soft tissues around major joints, particularly the hips, knees, elbows, and shoulders. Heterotopic ossification causes pain, limits joint range of motion, and interferes with positioning and movement. The mechanisms involve altered signaling from the injured brain that activates bone-forming cells in abnormal locations, increased inflammation, and changes in local blood flow (Long-term Consequences of TBI in Bone, 2018).pmc.ncbi.nlm.nih
Effects on Vital Organs
Traumatic brain injury extends its impact beyond the brain to affect vital organs throughout the body. This multiorgan dysfunction occurs through autonomic nervous system disruption, inflammatory mediators, hormonal changes, and metabolic alterations that the injured brain cannot properly regulate.
The cardiovascular system experiences significant effects following traumatic brain injury. Severe injuries trigger massive catecholamine release and autonomic nervous system activation, leading to elevated heart rate, increased blood pressure, and altered heart rhythm. While these changes may initially help maintain blood flow to the injured brain, they can become harmful if excessive or prolonged. Cardiac complications include neurogenic stress cardiomyopathy, where the heart muscle weakens temporarily; cardiac arrhythmias; and increased myocardial oxygen demand that can trigger ischemia in vulnerable individuals. Blood pressure dysregulation complicates management, as both very high and very low blood pressure can worsen brain injury outcomes (Multiorgan Dysfunction After Severe TBI, 2021).pmc.ncbi.nlm.nih
The pulmonary system suffers frequent complications after traumatic brain injury. Acute lung injury develops in many patients with severe brain trauma due to neurogenic pulmonary edema, where fluid accumulates in the lungs from autonomic nervous system dysfunction and altered blood vessel permeability. Pneumonia occurs frequently due to impaired ability to protect the airway, reduced cough effectiveness, and prolonged mechanical ventilation when required. Acute respiratory distress syndrome, a severe form of lung injury, can develop. These pulmonary complications reduce oxygen delivery to the injured brain and other organs, potentially worsening outcomes (Multiorgan Dysfunction After Severe TBI, 2021).pmc.ncbi.nlm.nih
The gastrointestinal system demonstrates vulnerability to traumatic brain injury effects. Autonomic nervous system disruption alters gut motility, reduces blood flow to intestinal tissues, and changes the gut microbiome composition. These changes increase intestinal permeability, potentially allowing bacteria and bacterial products to enter the bloodstream. Stress ulcers develop in the stomach and duodenum from reduced mucosal blood flow and altered protective mechanisms. Feeding intolerance complicates nutritional support. Gastrointestinal complications affect nutrient absorption, contribute to systemic inflammation, and may influence brain recovery (Multiorgan Dysfunction After Severe TBI, 2021).pmc.ncbi.nlm.nih
Kidney function becomes impaired in many traumatic brain injury patients through multiple mechanisms. Sympathetic nervous system activation reduces blood flow to the kidneys, decreasing glomerular filtration. Inflammatory mediators released from the injured brain affect kidney cells directly. Acute kidney injury develops in a significant proportion of patients with severe traumatic brain injury, potentially requiring dialysis and affecting long-term kidney function. Impaired kidney function complicates medication dosing, fluid management, and elimination of metabolic waste products (Multiorgan Dysfunction After Severe TBI, 2021).pmc.ncbi.nlm.nih
The liver, which synthesizes proteins and lipids crucial for brain recovery, experiences altered function following traumatic brain injury. Inflammatory signals affect hepatic protein synthesis, lipid metabolism, and glucose production. The liver may become a source of inflammatory mediators that worsen brain injury. Liver dysfunction affects drug metabolism, coagulation factor production, and nutritional status. Recent research suggests the liver plays a crucial role in traumatic brain injury pathogenesis through its metabolic and inflammatory functions (Traumatic brain injury from a peripheral axis perspective, 2025).sciencedirect
Metabolic and endocrine systems show widespread dysfunction after traumatic brain injury. The hypothalamic-pituitary axis, which regulates hormonal systems, commonly sustains damage. This results in deficiencies of growth hormone, thyroid hormone, adrenal hormones, and sex hormones. Growth hormone deficiency contributes to muscle wasting, bone loss, fatigue, and cognitive impairment. Thyroid hormone deficiency slows metabolism, affects mood and cognition, and impairs recovery. Adrenal insufficiency compromises stress response and blood pressure regulation. Sex hormone deficiencies affect mood, energy, muscle mass, and bone density. These hormonal disturbances can develop acutely or emerge months to years after injury, emphasizing the need for ongoing monitoring (Neuroendocrine Disturbances Following TBI, 2023).biausa
Blood sugar regulation becomes disrupted following traumatic brain injury, with both hyperglycemia and hypoglycemia occurring. The injured brain has altered glucose metabolism and increased metabolic demands. Insulin resistance can develop, affecting cellular energy metabolism throughout the body. These metabolic changes complicate nutritional management and may affect recovery outcomes. Evidence suggests that metabolic dysregulation contributes to cognitive impairment, as insulin and other metabolic hormones influence neuroplasticity and synaptic function (Metabolic hormones mediate cognition, 2009).sciencedirect
A TBI Symptom Questionnaire Example:
Detailed History and Questioning by Providers
Comprehensive assessment through detailed history-taking and systematic questioning forms the foundation of effective traumatic brain injury care. Both chiropractors and nurse practitioners use specific strategies to uncover cognitive impairment and identify the full scope of injury-related problems. A thorough history begins with understanding the mechanism of injury. Providers need detailed information about how the traumatic event occurred, including the forces involved, direction of impact, presence of acceleration or deceleration, rotational forces, and any loss of consciousness. This information helps predict injury patterns and potential complications. For example, motor vehicle accidents often cause both brain injury and cervical spine trauma, blast injuries affect multiple organ systems, and falls in older adults carry high risk for bleeding complications (Survey of chiropractic clinicians on MTBI, 2018).pmc.ncbi.nlm.nih
Timeline documentation provides essential context for symptom development. Providers should ask when symptoms first appeared, whether they emerged immediately after injury or developed gradually, how symptoms have changed over time, and whether any factors make symptoms better or worse. Some traumatic brain injury symptoms appear immediately, while others develop days, weeks, or months later. This temporal pattern helps distinguish primary injury effects from secondary complications and guides treatment planning (Survey of chiropractic clinicians on MTBI, 2018).pmc.ncbi.nlm.nih Cognitive symptoms require detailed exploration through specific questioning. Providers should systematically assess attention and concentration by asking about distractibility, ability to complete tasks, difficulty maintaining focus during conversations or activities, and need for frequent breaks. Memory problems should be explored across multiple domains, including difficulty remembering recent events, appointments, or conversations; problems with learning new information; struggles with recalling previously known facts or procedures; and concerns expressed by family members about changes in memory. Executive function difficulties often manifest as problems with planning, organizing, initiating tasks, managing time, making decisions, solving problems, and regulating emotions (Cognitive Problems After Traumatic Brain Injury, n.d.).uwmsktc.washington
Musculoskeletal symptoms deserve thorough investigation because they often accompany cognitive impairment and affect rehabilitation. Providers should ask about neck pain, back pain, headaches, dizziness, balance problems, muscle weakness, numbness or tingling, muscle stiffness or spasms, and changes in coordination or movement. The cervical spine frequently sustains injury concurrently with traumatic brain injury, and cervical dysfunction can contribute to headaches, dizziness, and cognitive symptoms through its effects on blood flow and proprioceptive input (Chiropractic Management of Post Traumatic Vertigo, 2004).pmc.ncbi.nlm.nih Vestibular symptoms require specific questioning because they are common but often underreported. Providers should directly ask about dizziness, vertigo, lightheadedness, imbalance, motion sensitivity, visual disturbances with movement, and situations that provoke symptoms. Many traumatic brain injury patients have vestibular dysfunction but do not report symptoms spontaneously, possibly because brain injury affects symptom perception. Direct questioning reveals these problems that might otherwise remain unidentified (Vestibular dysfunction in acute TBI, 2019).pmc.ncbi.nlm.nih
Visual symptoms affect the majority of traumatic brain injury patients and significantly impact function. Providers should systematically assess blurred vision, double vision, difficulty focusing, eye strain, light sensitivity, problems tracking moving objects, difficulty with reading, visual field deficits, and eye misalignment. Because visual dysfunction contributes to balance problems, reading difficulties, and participation limitations, thorough visual assessment guides appropriate referrals and treatment planning (Eye Movement Problems After Brain Injury, 2021).optometrists Sleep disturbances occur in thirty to seventy percent of traumatic brain injury patients and affect recovery. Providers should ask about difficulty falling asleep, frequent nighttime awakenings, early morning awakening, excessive daytime sleepiness, prolonged sleep need, nightmares, and changes in sleep schedule or quality. Sleep disruption worsens cognitive function, mood, pain perception, and overall recovery. Identifying sleep problems allows targeted interventions that may improve multiple outcome domains (Sleep Disorders After Brain Injury, 2025).practicalneurology
Mood and emotional symptoms commonly develop after traumatic brain injury and require sensitive, direct questioning. Depression affects forty to sixty percent of individuals with moderate to severe traumatic brain injury. Symptoms include persistent sadness, loss of interest in previously enjoyed activities, feelings of hopelessness, changes in appetite, sleep disturbances, fatigue, difficulty concentrating, and suicidal thoughts. Anxiety disorders affect eleven to seventy percent of traumatic brain injury patients, with symptoms including excessive worry, restlessness, tension, hypervigilance, and panic attacks. Emotional dysregulation may manifest as irritability, anger outbursts, emotional lability, or apathy (Mood Disorders Following TBI, 2025).practicalneurology
Functional impacts should be thoroughly explored to understand how symptoms affect daily life. Providers should ask about changes in work or school performance, difficulty managing household tasks, problems maintaining relationships, challenges with self-care activities, driving limitations, and overall quality of life. Understanding functional limitations helps prioritize treatment goals and measure progress over time. Family member or caregiver input provides valuable perspective on functional changes that patients may not fully recognize (Strategies Nurses Use when Caring for Patients with TBI, 2019).pmc.ncbi.nlm.nih Inquiry about significant others’ observations proves particularly valuable, as cognitive impairment can affect self-awareness. Studies show that seventy to eighty-eight percent of healthcare providers inquire about family members’ observations of cognitive changes. Family members often notice personality changes, memory problems, emotional shifts, and functional declines that patients minimize or do not recognize (Survey of chiropractic clinicians on MTBI, 2018).pmc.ncbi.nlm.nih
Associated Symptoms from TBI
Beyond cognitive impairment, traumatic brain injury produces a constellation of associated symptoms that significantly affect quality of life and recovery. Understanding these symptoms helps providers develop comprehensive treatment approaches and set realistic expectations for recovery.
Fatigue represents one of the most common and debilitating symptoms after traumatic brain injury. Research indicates that as many as ninety-eight percent of people who have experienced traumatic brain injury have some form of fatigue. This fatigue differs from normal tiredness in that it does not improve adequately with rest, appears disproportionate to activity level, and significantly limits function. Physical fatigue manifests as muscle weakness, reduced endurance, and increased need for rest. Mental fatigue involves reduced ability to sustain cognitive effort, difficulty concentrating as the day progresses, and overwhelming sense of mental exhaustion. Fatigue worsens other symptoms, including pain, cognitive problems, and mood disturbances (Fatigue After Brain Injury, 2021).biausa
Headaches affect up to eighty percent of traumatic brain injury survivors and may persist for months or years. Post-traumatic headaches take various forms, including tension-type headaches characterized by band-like pressure, migraine-type headaches with throbbing pain and associated symptoms, cervicogenic headaches originating from neck dysfunction, and neuralgic headaches involving specific nerve distributions. Headaches interfere with concentration, sleep, mood, and participation in rehabilitation activities. The mechanisms involve inflammation, altered pain processing, muscle tension, cervical spine dysfunction, and vascular changes (Traumatic Brain Injury, 2023).ninds.nih
Sleep disorders affect thirty to seventy percent of traumatic brain injury patients and take various forms. Insomnia, characterized by difficulty initiating or maintaining sleep, affects approximately twenty-nine percent of patients. Sleep apnea, where breathing repeatedly stops during sleep, occurs in about twenty-five percent. Hypersomnia, excessive sleepiness or prolonged sleep need, affects twenty-eight percent. Narcolepsy develops in approximately four percent. These sleep disturbances result from damage to brain structures regulating sleep-wake cycles, hormonal disruptions affecting sleep, pain interfering with rest, and mood disturbances. Poor sleep quality worsens cognitive function, mood, pain, fatigue, and overall recovery (Impact of TBI on sleep, 2019).pmc.ncbi.nlm.nih
Depression emerges as a frequent complication, affecting thirteen to fifty-three percent of traumatic brain injury survivors. Post-traumatic depression may result from direct brain damage affecting mood-regulating circuits, particularly in frontotemporal regions, or from psychological response to injury-related losses and life changes. Symptoms include persistent sadness, loss of interest, feelings of worthlessness, guilt, changes in appetite and sleep, fatigue, difficulty concentrating, psychomotor agitation or retardation, and suicidal ideation. Depression significantly impairs rehabilitation participation, functional recovery, and quality of life. It increases caregiver burden and raises risk of suicide (Mood Disorders Following TBI, 2025).pmc.ncbi.nlm.nih+1
Anxiety disorders develop in eleven to seventy percent of traumatic brain injury patients. Post-traumatic stress disorder occurs particularly in those whose injuries resulted from violence, combat, or accidents. Generalized anxiety disorder involves excessive, uncontrollable worry about multiple life domains. Panic disorder includes unexpected panic attacks with physical symptoms like rapid heartbeat, sweating, trembling, and fear of dying. Social anxiety involves fear of social situations and negative evaluation. Anxiety often co-occurs with depression and exacerbates cognitive symptoms, sleep problems, and pain (Anxiety and Depression Following TBI, 2023).connectivity+1
Irritability and emotional dysregulation commonly follow traumatic brain injury, resulting from damage to frontal lobe regions that regulate emotions and control impulses. Individuals may experience frequent anger, decreased frustration tolerance, emotional outbursts disproportionate to triggers, rapid mood shifts, and difficulty calming down once upset. These symptoms strain relationships, interfere with community reintegration, and may limit employment options (Traumatic brain injury and mood disorders, 2020).pmc.ncbi.nlm.nih
Sensory sensitivities develop in many traumatic brain injury survivors. Light sensitivity, or photophobia, makes normal lighting uncomfortable and can trigger headaches. Noise sensitivity causes ordinary sounds to seem overwhelmingly loud or irritating. Some individuals develop increased sensitivity to touch, temperature, or smells. These sensitivities result from altered sensory processing in the injured brain and often accompany headaches and cognitive symptoms. They limit participation in bright or noisy environments and affect quality of life (Traumatic Brain Injury, 2023).ninds.nih
Beyond the Surface: Understanding the Effects of Personal Injury- Video
Integrative Approach: Chiropractic and Nurse Practitioner Care
An integrative approach combining chiropractic care with nurse practitioner oversight offers comprehensive support for individuals recovering from traumatic brain injuries. This collaborative model addresses the complex, multifaceted nature of brain injury by bringing together complementary expertise and treatment approaches. Chiropractic care focuses on the nervous system and musculoskeletal health through manual therapies, rehabilitative exercises, and supportive interventions. Chiropractors assess and address spinal alignment, particularly in the cervical spine which commonly sustains injury alongside traumatic brain injury. Cervical spine dysfunction contributes to many post-traumatic brain injury symptoms, including headaches, neck pain, dizziness, balance problems, and potentially cognitive symptoms through effects on blood flow and proprioceptive input (Chiropractic Care Supports TBI Healing, 2009).pinnaclehealthchiro
Spinal adjustments form a core component of chiropractic care for traumatic brain injury patients. These precise, controlled movements applied to spinal joints aim to restore proper alignment, reduce nerve interference, and optimize nervous system function. In the cervical spine, adjustments may improve blood flow to the brain by reducing compression on vertebral arteries. Research demonstrates that correction of cervical lordosis associates with immediate increases in cerebral blood flow, suggesting that biomechanical improvements can positively affect brain perfusion (Cervical lordosis correction increases cerebral blood flow, 2019).pmc.ncbi.nlm.nih
Chiropractic care addresses cerebrospinal fluid circulation, which plays important roles in brain health and recovery. Cerebrospinal fluid protects and nourishes the brain, removes metabolic waste products, and facilitates nutrient delivery. Traumatic brain injury can disrupt normal cerebrospinal fluid flow. Manual chiropractic techniques and spinal adjustments may help restore optimal cerebrospinal fluid dynamics, supporting brain healing processes (Chiropractic Care Supports TBI Healing, 2009).pinnaclehealthchiro
Soft tissue therapies complement spinal adjustments by addressing muscle tension, fascial restrictions, and myofascial pain that commonly develop after trauma. Techniques include manual therapy, instrument-assisted soft tissue mobilization, therapeutic massage, and trigger point release. These interventions reduce pain, improve tissue quality, restore range of motion, and promote healing. Addressing soft tissue dysfunction proves particularly important for cervical and upper thoracic regions where muscle tension contributes to headaches and affects cervical spine mechanics (Chiropractic Care Supports TBI Healing, 2009).elpasochiropractorblog+1
Rehabilitative exercises form an essential component of chiropractic traumatic brain injury care. Exercise programs address specific deficits identified through comprehensive assessment. Cervical strengthening and stabilization exercises improve neck muscle function and support spinal structures. Vestibular rehabilitation exercises help retrain balance systems through specific movements and visual tasks. Oculomotor exercises address eye tracking and coordination problems. Proprioceptive training improves body position awareness and motor control. Progressive strengthening builds overall fitness and supports functional recovery (Therapeutic Interventions for TBI, 2024).physio-pedia
Chiropractic neurologists employ specialized techniques to stimulate nervous system recovery. These approaches use specific sensory inputs, including light, sound, movement, and other stimuli, to activate targeted brain regions and promote neuroplasticity. The principle recognizes that the brain responds to appropriate stimulation similarly to how muscles respond to exercise, strengthening neural pathways through repeated activation. This non-invasive approach may benefit patients who have not responded well to traditional treatments (Chiropractic Neurology Supports Brain Healing, 2025).hmlfunctionalcare+1 Nurse practitioners provide medical oversight and management that complements chiropractic interventions. As board-certified family practice nurse practitioners with advanced training, they perform comprehensive health assessments, order and interpret diagnostic tests, prescribe medications when appropriate, manage medical comorbidities, and coordinate care across specialties. This medical oversight ensures that serious complications are identified and addressed promptly while supporting the body’s natural healing processes (Dr. Alex Jimenez’s Integrative Practice, n.d.).missionlegalcenter
Cognitive support represents an important aspect of nurse practitioner care for traumatic brain injury patients. Nurse practitioners assess cognitive function using standardized tools, provide education about cognitive symptoms and compensatory strategies, recommend cognitive rehabilitation services, and monitor cognitive recovery over time. They help patients and families understand cognitive changes and develop practical approaches to manage daily activities despite cognitive limitations (Strategies Nurses Use when Caring for Patients with TBI, 2019).nursing.duke+1
Metabolic and nutritional support provided by nurse practitioners addresses the altered metabolic demands following traumatic brain injury. The injured brain has increased energy requirements and specific nutritional needs. Nurse practitioners assess nutritional status, develop individualized nutrition plans, recommend supplements when indicated, and monitor response to nutritional interventions. Emerging research suggests that specific nutrients, including omega-3 fatty acids, vitamin D, magnesium, and amino acids, may support brain recovery when provided during the acute and subacute phases after injury (Nutritional interventions to support acute mTBI recovery, 2022).frontiersin
Emotional and psychological support forms another critical component of nurse practitioner care. They screen for depression, anxiety, post-traumatic stress disorder, and other mood disturbances, provide counseling and supportive therapy, prescribe psychotropic medications when appropriate, and refer to mental health specialists when needed. Addressing emotional health proves essential for overall recovery, as mood disturbances affect rehabilitation participation, cognitive function, and quality of life (Mood Disorders Following TBI, 2025).practicalneurology
Sleep management represents an area where nurse practitioner expertise particularly benefits traumatic brain injury patients. Nurse practitioners assess sleep quality and quantity, identify specific sleep disorders, recommend sleep hygiene improvements, prescribe sleep aids when appropriate, and coordinate sleep studies when indicated. Improving sleep quality enhances cognitive function, mood, pain management, and overall recovery (Sleep Disorders After Brain Injury, 2025).practicalneurology
The integrative model exemplified by Dr. Alexander Jimenez’s dual-scope practice demonstrates how chiropractic and nurse practitioner expertise can be combined within a single provider or collaborative team. Dr. Jimenez’s approach incorporates functional medicine principles, detailed health assessments, spinal and musculoskeletal care, nutritional support, exercise therapy, and comprehensive medical case management. This holistic model addresses the person as a whole rather than treating isolated symptoms, potentially leading to more complete and sustained recovery (Dr. Alex Jimenez’s Integrative Practice, n.d.).elpasochiropractorblog+1
Holistic Treatment Plans
Comprehensive, holistic treatment plans for traumatic brain injury incorporate multiple therapeutic approaches that address physical, cognitive, emotional, and metabolic aspects of recovery. These plans recognize that healing requires supporting the body’s natural recovery mechanisms while addressing specific symptoms and functional limitations.
Initial assessment forms the foundation of effective treatment planning. Comprehensive evaluation includes detailed history of the injury and symptom development, neurological examination assessing mental status, cranial nerves, motor function, sensory function, reflexes, coordination, and gait. Cervical spine assessment evaluates posture, range of motion, segmental mobility, muscle tone and strength, and joint function. Vestibular and oculomotor testing examines balance, eye movements, and visual-vestibular integration. Cognitive screening identifies attention, memory, processing speed, and executive function deficits. Mood and sleep questionnaires quantify emotional and sleep-related symptoms (Hidden TBI Symptoms: Integrative Model, 2025).elpasochiropractorblog
Spinal care targets cervical and upper thoracic dysfunction that commonly accompanies traumatic brain injury. Treatment begins with gentle mobilization techniques before progressing to specific adjustments as tolerated. The approach remains cautious, individualized, and responsive to patient symptoms, as excessive or aggressive treatment could worsen symptoms in vulnerable patients. Spinal adjustments aim to restore proper alignment, reduce nerve interference, improve proprioceptive input, and enhance blood flow to the brain. Treatment frequency and intensity adapt based on patient response, with some individuals benefiting from frequent initial visits that taper as function improves (Hidden TBI Symptoms: Integrative Model, 2025).zakerchiropractic+1
Soft tissue interventions address muscle tension, trigger points, fascial restrictions, and movement dysfunction. Manual therapy techniques include ischemic compression for trigger points, myofascial release for fascial restrictions, instrument-assisted soft tissue mobilization to address tissue quality, and therapeutic massage for overall relaxation and pain relief. These interventions reduce pain, improve tissue flexibility, restore normal movement patterns, and support overall healing. Treatment focuses particularly on cervical, upper thoracic, and cranial regions where soft tissue dysfunction contributes to headaches, neck pain, and dizziness (Hidden TBI Symptoms: Integrative Model, 2025).elpasochiropractorblog
Exercise therapy progresses systematically based on symptom tolerance and functional goals. Early-phase exercises focus on gentle range of motion, postural awareness, and basic strengthening within symptom limits. As tolerance improves, exercises advance to include cervical stabilization training to support injured structures, vestibular rehabilitation exercises to retrain balance systems, oculomotor exercises to improve eye coordination and tracking, proprioceptive training to enhance body position awareness, and progressive aerobic and strengthening exercises to build overall fitness. Exercise prescription follows graduated principles, starting with brief, low-intensity activities and progressing gradually while monitoring for symptom exacerbation (Hidden TBI Symptoms: Integrative Model, 2025).elpasochiropractorblog
Nutritional support addresses the increased metabolic demands and specific nutrient needs following traumatic brain injury. The injured brain requires adequate calories, high-quality protein for tissue repair, essential fatty acids particularly omega-3s for neural membrane health and anti-inflammatory effects, antioxidants to combat oxidative stress, vitamins and minerals for metabolic processes and neurotransmitter synthesis, and adequate hydration for optimal brain function. Nutritional assessment identifies deficiencies and guides supplement recommendations. Evidence suggests that omega-3 fatty acids, vitamin D, magnesium, and certain amino acids may support brain recovery when provided during acute and subacute phases (Nutritional interventions to support acute mTBI recovery, 2022).pmc.ncbi.nlm.nih+1
Cognitive rehabilitation strategies help individuals compensate for cognitive impairments and retrain affected abilities. Techniques include external memory aids such as written schedules, calendars, lists, and electronic reminders; attention strategies like reducing distractions, taking breaks, and focusing on one task at a time; organization systems that simplify and structure tasks; time management tools that help with planning and prioritization; and specific cognitive exercises that challenge and strengthen affected abilities. Education helps patients and families understand cognitive changes and develop realistic expectations while maintaining hope for continued improvement (Strategies Nurses Use when Caring for Patients with TBI, 2019).nursing.duke+1
Sleep optimization represents a crucial treatment component that affects multiple outcome domains. Sleep hygiene education covers maintaining consistent sleep-wake schedules, creating optimal sleep environments that are dark, quiet, and cool, limiting screen time before bed, avoiding caffeine and alcohol, and using relaxation techniques. Treatment of specific sleep disorders may include continuous positive airway pressure for sleep apnea, repositioning techniques for positional sleep disorders, or medications when appropriate. Improving sleep quality enhances cognitive function, mood, pain management, and overall recovery (Sleep Disorders After Brain Injury, 2025).practicalneurology
Pain management employs multiple modalities to address headaches, neck pain, and other pain complaints. Non-pharmacological approaches include manual therapy, therapeutic exercise, heat or cold application, relaxation techniques, and biofeedback. Pharmacological options when needed include appropriate analgesics, muscle relaxants, or nerve pain medications, used cautiously to avoid medication overuse and unwanted side effects. The goal emphasizes restoring function and reducing pain interference rather than complete pain elimination, which may not be achievable (Pain and Traumatic Brain Injury, 2024).health
Mood and emotional support acknowledges the profound psychological impacts of brain injury and chronic symptoms. Interventions include supportive counseling addressing adjustment to injury and life changes, cognitive-behavioral therapy to modify unhelpful thought patterns and behaviors, stress management techniques, mindfulness and relaxation training, support groups connecting individuals with others facing similar challenges, and psychiatric medications when appropriate. Family involvement and education play a crucial role in creating a supportive home environment that fosters recovery from mood disorders following traumatic brain injury (TBI) (Mood Disorders Following TBI, 2025).practicalneurology
Coordination across providers ensures comprehensive, efficient care. Regular communication between chiropractors, nurse practitioners, physical therapists, occupational therapists, speech-language pathologists, neuropsychologists, and other specialists involved in care promotes integrated treatment planning. Case conferences discuss patient progress, treatment responses, and plan modifications. This team approach prevents fragmented care and ensures all providers work toward shared goals. Dr. Alexander Jimenez’s practice exemplifies this coordination by offering multiple services within an integrated setting while maintaining referral relationships with specialists for needs beyond the clinic’s scope (Dr. Alex Jimenez’s Integrative Practice, n.d.).missionlegalcenter
Progress monitoring uses both objective measures and subjective reports to assess treatment effectiveness. Standardized outcome measures track symptom severity, functional abilities, and quality of life over time. Regular reassessments identify improvements, plateaus, or declines that necessitate adjustments to treatment. Flexible treatment plans adapt to changing needs as recovery progresses, with some interventions becoming less necessary as function improves, while others may need to be added or intensified. This responsive approach ensures that treatment remains appropriate throughout the recovery trajectory.
Conclusion
Through disturbed neuronal regulation, inflammatory processes, hormonal imbalances, and metabolic alterations, traumatic brain injury is a complicated medical disorder that affects not just the brain but the whole body. One of the most significant effects is cognitive impairment, which affects executive function, processing speed, memory, attention, and other mental skills essential for independent living. Autonomic dysfunction and systemic inflammatory reactions affect essential organs, whereas spasticity, weakness, coordination issues, and balance deficiencies affect the musculoskeletal system. Comprehensive treatment for traumatic brain injury requires an understanding of the brain-body link. Injury disrupts the complex communication networks that connect the brain to muscles, bones, organs, and metabolic systems, resulting in far-reaching impacts that necessitate a variety of therapeutic modalities. Healthcare professionals can identify the complete range of injury-related issues, including cognitive impairments that patients may not voluntarily mention and musculoskeletal or systemic symptoms that have a substantial impact on recovery, by obtaining a thorough history and asking methodical questions.
The multifaceted character of traumatic brain injury rehabilitation is addressed by an integrated strategy that combines chiropractic treatment with nurse practitioner supervision. Through soft tissue treatments, spinal adjustments, and rehabilitative activities that enhance biomechanics, lessen pain, and promote neuroplasticity, chiropractic interventions restore nervous system function. Nurse practitioners provide comprehensive care, including mood management, dietary counseling, medical supervision, cognitive support, and complete care coordination. Dr. Alexander Jimenez’s dual-scope practice exemplifies how this teamwork yields comprehensive treatment regimens that address the mental, emotional, physical, and metabolic aspects of recovery. Holistic treatment regimens include multiple therapy modalities that are customized to each patient’s specific needs and modified in response to those needs. While targeting specific symptoms and functional constraints, these programs recognize that promoting the body’s natural healing processes is crucial to a successful recovery. To promote healing and restore function, various therapies work in concert, including spinal care, soft tissue work, exercise therapy, nutritional assistance, cognitive rehabilitation, sleep optimization, pain management, and emotional support. Throughout the rehabilitation process, interventions are tailored to individual progress via progress tracking and therapeutic adaptability. Depending on a variety of circumstances, including age, location, severity of the damage, and pre-accident health, each person’s road to recovery from traumatic brain injury is unique. Some individuals heal very quickly and completely, while others have long-term functional impairments and lingering symptoms. By treating the whole person rather than just specific symptoms and by promoting the brain’s extraordinary ability to adapt and recover, an integrated, holistic approach gives promise for better results. Recovery prospects for those dealing with traumatic brain injury are expected to be substantially enhanced by ongoing research, better diagnostic instruments, and improved treatment modalities.
Collins, M. E., & Misukanis, T. M. (2004). Chiropractic Management of a Patient with Post-Traumatic Vertigo of Complex Origin. Journal of Chiropractic Medicine, 4(4), 32-38. https://pmc.ncbi.nlm.nih.gov/articles/PMC2647031/
Figueiredo, T. H., et al. (2024). An integrative, holistic treatment approach for veterans with chronic traumatic brain injury and associated comorbidities: case report. Frontiers in Neurology. https://pmc.ncbi.nlm.nih.gov/articles/PMC12081389/
Kanayama, G., et al. (2019). Increase in cerebral blood flow indicated by increased cerebral arterial area and pixel intensity on brain magnetic resonance angiogram following correction of cervical lordosis. Brain Circulation, 5(1), 19-26. https://pmc.ncbi.nlm.nih.gov/articles/PMC6458772/
Oyesanya, T. O., & Thomas, M. A. (2019). Strategies Nurses Use when Caring for Patients with Moderate-to-Severe Traumatic Brain Injury who have Cognitive Impairments. Journal of Clinical Nursing, 28(23-24), 4277-4289. https://pmc.ncbi.nlm.nih.gov/articles/PMC6800766/
Willing, A. E., et al. (2020). Potential of mesenchymal stem cells alone, or in combination, to treat traumatic brain injury. CNS Neuroscience & Therapeutics, 26(6), 616-627. https://pmc.ncbi.nlm.nih.gov/articles/PMC7248541/
Traumatic Brain Injury & Posture: From Subtle Balance Changes to Abnormal Posturing — and How Integrative Chiropractic Care Can Help
Traumatic brain injuries (TBIs) can quietly change how you balance and stand, even months after a mild concussion. In the most serious cases, TBIs can trigger rigid reflex body positions called decorticate or decerebrate posturing, which are medical emergencies. These posture changes often stem from problems in how the brain uses sensory, visual, and vestibular (inner ear) signals. Neck and upper-back (cervical and upper thoracic) strain can exacerbate the problem by disrupting head-neck alignment and irritating nerves, which may worsen headaches and dizziness. An integrative plan that includes medical oversight, chiropractic adjustments, and sensory–motor therapies may help restore better alignment, reduce symptom drivers, and support safer balance over time (as part of a team approach). Mount Sinai Health System+3braininjurycanada.ca+3Brain Injury Association of America+3
Why TBIs Affect Posture
The brain’s balance triangle: vision, vestibular system, and body sense
Good balance depends on three main inputs working together: eyes (vision), the inner ear (vestibular system), and proprioception (your body’s internal sense of position). After a TBI, even a mild one, the brain may process these signals less efficiently. That can leave you feeling unsteady, dizzy, or “off,” especially during walking, turning the head, or in busy visual settings (like grocery aisles). Large groups of people with brain injuries report issues with balance, showing how common this problem can be. (Brain Injury Canada explains that balance integrates strength, vision, and inner-ear function and that balance problems are frequently reported after brain injury.) braininjurycanada.ca
Mild TBI: subtle but persistent postural-control changes
Research reviews show that after a concussion, people can have lingering deficits in postural control that routine tests sometimes miss. Nonlinear balance metrics and instrumented measures can detect differences even when symptoms appear to be improved. In other words, you might feel “almost fine,” but objective measures still pick up changes in sway, gait, or dynamic stability. PMC+1
Moderate to severe TBI: larger balance impairments
In moderate-to-severe TBI, studies document more obvious balance asymmetries and mobility limitations, which often require targeted, progressive rehab to improve safety and independence. OUP Academic
When Posture Becomes an Emergency: Abnormal Posturing
In rare but severe brain injuries, the body can assume reflex, rigid positions that signal deep brain dysfunction and require immediate medical care.
Decorticate posturing: arms flexed toward the chest with clenched fists; legs extended and rigid. It’s a sign of serious brain damage affecting pathways in the cerebral cortex, thalamus, or upper midbrain. Call emergency services at once if you see this. (Cleveland Clinic; Mount Sinai.) Cleveland Clinic+1
Decerebrate posturing: arms and legs extended, toes pointed down, head/neck arched backward, with rigid muscles—often linked to lower midbrain or pontine involvement. This also demands urgent care. (Cleveland Clinic; Mount Sinai.) Cleveland Clinic+1
Abnormal posturing is typically evaluated in conjunction with other signs using tools such as the Glasgow Coma Scale (GCS) during emergency assessments. NCBI
The Neck–Brain Link: How Cervical and Upper Thoracic Issues Can Worsen Symptoms
TBIs often occur with whiplash or neck strain, which can disturb joint motion, muscle tone, and head-on-neck position. In some patients, this can contribute to cervicogenic dizziness, headaches, and neck-related balance problems—especially when turning the head or maintaining upright posture. Clinical discussions from Dr. Jimenez’s team describe how cervical dysfunction and upper thoracic stiffness may aggravate dizziness and balance challenges after head/neck trauma. El Paso, TX Doctor Of Chiropractic+2El Paso, TX Doctor Of Chiropractic+2
Dr. Jimenez, DC, APRN, FNP-BC, emphasizes that a careful examination of posture, cervical range of motion, and joint motion can reveal overlooked factors contributing to headaches and dizziness, and that progress often includes cervical stabilization and vestibular drills, alongside other care. El Paso, TX Doctor Of Chiropractic+1
What Symptoms Might You Notice?
Feeling wobbly, light-headed, or “tilted,” especially in visually busy places
Headaches (often starting at the neck or base of the skull), neck pain, and eye strain
Dizziness when turning the head, rolling in bed, or after long screen time
Fatigue, brain fog, or irritability that worsens as the day goes on
Slower walking, shorter steps, or veering off line
These align with common post-concussion complaints (headache, dizziness, fatigue) and with mobility/balance challenges described in the brain-injury literature. PMC+1
Symptom Questionnaire:
How Integrative Chiropractic Care Can Fit Into a TBI Recovery Plan
Important: Chiropractic care does not treat the brain injury itself and should not replace medical diagnosis or urgent care. It may, however, support symptom management and functional recovery when coordinated with your medical team (neurology, primary care, vestibular/physical therapy). Bergeron Clifford LLP
1) Restoring better spinal mechanics and alignment (especially upper neck)
Gentle, carefully selected spinal adjustments can reduce joint restrictions and muscle guarding in the cervical and upper thoracic regions. For some patients, improving head–neck alignment can reduce neck-related headaches and dizziness, which can indirectly improve balance and posture. Dr. Jimenez’s clinical materials and other chiropractic sources describe these goals and report symptom relief in select cases where the neck is a contributing factor. El Paso, TX Doctor Of Chiropractic+2El Paso, TX Doctor Of Chiropractic+2
2) Supporting neurophysiology and fluid dynamics (theoretical/adjunctive)
Some clinics note that adjustments may improve blood and cerebrospinal fluid (CSF) circulation, potentially aiding brain recovery by optimizing the environment around neural tissue. The evidence here is preliminary and should be framed as “may help” within a broader rehabilitation plan; still, it’s a common adjunctive rationale in clinical practice. Impact Medical Group+1
3) Sensory–motor rehabilitation to rebuild coordination
Integrative chiropractic and functional-neurology clinics often pair adjustments with targeted sensory and movement therapies: gaze stabilization, saccade/pursuit drills, balance progressions (wide base → narrow base → head turns), dual-task walking, and cervical proprioception exercises. These aim to retrain the brain (neuroplasticity) and calibrate vision–vestibular–proprioceptive inputs. HML Functional Care
4) Team-based care improves outcomes and safety
Medical guidance identifies red flags, rules out dangerous causes, and directs imaging or vestibular testing when needed. Rehabilitation professionals measure postural control, gait, and mobility using validated tools to demonstrate progress over time. Observational and review data indicate that balance changes occur after concussion, supporting the need for a structured assessment to guide rehabilitation. PMC+1
A Step-By-Step Care Pathway (What This Can Look Like)
Medical evaluation first (especially if symptoms are new, severe, or worsening). Providers check for red flags and determine whether urgent care or imaging is necessary. Abnormal posturing = emergency.Mount Sinai Health System+1
Cervical and upper thoracic care: gentle mobilization/adjustments (as appropriate), soft-tissue work, and home exercises to restore motion and reduce headache/neck-related dizziness. El Paso, TX Doctor Of Chiropractic
Sensory–motor retraining: vestibular and oculomotor drills, graded balance tasks, gait training; progress in small, safe steps. HML Functional Care
Lifestyle and pacing: sleep, graded activity, hydration, and symptom-paced screens/exercise—often supported by nurse-practitioner-led coaching in integrative settings. (Dr. Jimenez’s practice materials emphasize whole-person plans and steady progression.) El Paso, TX Doctor Of Chiropractic
How TBIs Can Lead to Spinal Misalignments and Symptom Flares
Impact mechanics (falls, crashes, sports) can strain facet joints, discs, and deep neck muscles.
The body may then adopt protective postures (chin jutting, shoulder guarding), which can irritate cervical nerves and muscle trigger points.
These patterns may worsen headaches and dizziness by disturbing cervical proprioception and upper-neck mobility—especially around C0–C2, a frequent source of cervicogenic symptoms after whiplash/TBI. Clinical articles on cervicogenic dizziness echo these links and suggest appropriate manual care and stabilization when indicated (after medical clearance). El Paso, TX Doctor Of Chiropractic+1
When Symptoms Become “Rigid Posturing”
Remember: decorticate or decerebrate posturing means severe brain dysfunction. The person is typically unconscious and in a coma; both patterns require 911/emergency care now. (Do not attempt chiropractic or rehab; call for medical help immediately.) Cleveland Clinic+1
Tests and Tools for TBI & Postural Problems (From Simplest to Most Advanced)
Note: Your exact pathway depends on symptoms and safety. Start with medical evaluation and add tests as needed.
Bedside & Screening (simplest)
History and neuro exam (headache, dizziness, nausea, vision changes, sleep, mood, neck pain; cranial nerves; coordination).
Glasgow Coma Scale (GCS) in acute settings to rate eye, verbal, and motor responses. NCBI
Symptom scales (e.g., post-concussion symptom checklists). Mayo Clinic
Basic balance screens (Romberg, tandem stance, timed up-and-go), and observation of gait and turns.
Cervical exam: range of motion, segmental motion, palpation, and joint position error tests for proprioception when appropriate. (Dr. Jimenez highlights posture and cervical mechanics in clinical content.) El Paso, TX Doctor Of Chiropractic
Clinic-level functional tests
BESS (Balance Error Scoring System) and instrumented postural sway for more sensitive detection of balance deficits after concussion. PMC
Community Balance & Mobility Scale (CB&M) for higher-level balance and mobility challenges (validated in brain injury populations). PMC
Cervical/vestibular differentiation tests (to help sort inner-ear vs. neck-driven dizziness).
Specialized vestibular & ocular testing
Videonystagmography (VNG), calorics, rotary chair, and dynamic visual acuity tests to quantify vestibular deficits.
Eye-tracking or computerized oculomotor measures for pursuit/saccades.
Computerized posturography/force-plate is utilized for objective sway and strategy analysis, while center-of-mass measures aid in characterizing dynamic postural control following a concussion. IJSPT
Neurocognitive assessment
Standardized tests of attention, processing speed, memory, and executive function are used in concussion management (clinic-dependent).
Imaging & electrophysiology (advanced)
CT (acute bleed/fracture) and MRI (structural injury).
Diffusion Tensor Imaging (DTI) (white-matter pathways) and functional MRI in research/selected clinical contexts.
EEG if seizures or atypical episodes are suspected. (Mount Sinai lists EEG among tests for abnormal posturing workups; emergency pathways decide timing.) Mount Sinai Health System+1
PET/SPECT in select specialty centers; blood biomarkers (e.g., GFAP, UCH-L1) may be used in emergency algorithms.
Evidence Snapshots: What Research and Clinical Sources Say
Postural control can remain impaired after concussion; sophisticated metrics can reveal deficits not obvious on quick screens. PMC
Dynamic postural control, as measured by center-of-mass, is a useful outcome within one year post-concussion. IJSPT
Balance limitations after TBI are common and affect independence; better sitting balance early in rehab predicts better self-care after discharge. Brain Injury Association of America
Cervicogenic dizziness and neck-related headache can follow whiplash/head trauma; carefully managed manual therapy and cervical stabilization may reduce symptom drivers. (Clinical sources, including Dr. Jimenez’s site.) El Paso, TX Doctor Of Chiropractic+1
Chiropractic care should be adjunctive—not a replacement for medical treatment—and may help selected patients as part of a team plan, especially when cervical dysfunction contributes to symptoms. Bergeron Clifford LLP
Some clinics suggest that adjustments may help with blood and cerebrospinal fluid flow; however, this idea remains a theory and should be clearly explained to patients and used as part of a medically supervised plan. Impact Medical Group+1
A Practical, Integrated Plan (Example)
Built around safety, simplicity, and steady progress—and coordinated with your medical team.
Protect & screen: See a clinician first. Urgent signs (worsening severe headache, repeated vomiting, loss of consciousness, new weakness/vision loss, abnormal posturing) need emergency care. Mount Sinai Health System+1
Calm the neck: Gentle manual therapy and mobility work for the cervical/upper thoracic regions to reduce joint restriction and muscle guarding. Add home drills (chin nods, scapular setting, breathing) and progress slowly. El Paso, TX Doctor Of Chiropractic
Recalibrate balance systems: Start with a wide-base stance, eyes open → eyes closed; then narrow base; then add head turns and dual-task steps. Integrate gaze stabilization (VOR) and visual motion tolerance exercises as symptoms allow. HML Functional Care
Train real-life tasks: Gentle walking on level ground → turns → uneven terrain; keep sessions short and frequent. Measure progress with CB&M or instrumented sway when available. PMC
Whole-person support: Sleep regularity, hydration, anti-inflammatory nutrition, and pacing (breaks between screens/reading). Clinics like Dr. Jimenez’s emphasize collaborative care—chiropractic care, nurse practitioner oversight, and vestibular/physical therapy—ensuring each domain is covered. El Paso, TX Doctor Of Chiropractic
When to Call Right Away (Red Flags)
Abnormal posturing (decorticate/decerebrate), severe confusion, or unresponsiveness
Worsening severe headache, repeated vomiting, seizures, new weakness/numbness, or vision loss
Neck pain with fever, sudden stiff neck, or neurological deficits
How Dr. Alexander Jimenez’s Team Applies This Locally (El Paso)
Dr. Jimenez, DC, APRN, FNP-BC, highlights a dual-scope approach: identifying cervical drivers of headache/dizziness, rebuilding posture with gentle adjustments and stabilization, and combining this with vestibular drills, balance progressions, and lifestyle support. His clinical articles emphasize the importance of careful posture and cervical motion exams, stepwise progress, and collaborative plans with medical and rehabilitation partners. El Paso, TX Doctor Of Chiropractic+1
The Bottom Line
Mild TBI can leave behind subtle balance problems; severe TBI can cause abnormal posturing—an emergency. PMC+2Cleveland Clinic+2
These changes stem from how the brain integrates vision, vestibular input, and body sense, and they can be worsened by neck/upper-back dysfunction. braininjurycanada.ca+1
Integrative care—encompassing medical oversight, targeted chiropractic adjustments for cervical mechanics, and sensory–motor rehabilitation—offers a practical path to safer posture and stability. HML Functional Care+1
Inness, E. L., et al. (2011). [Measuring balance and mobility after traumatic brain injury: Validation of the Community Balance and Mobility Scale (CB&M)]. Journal of Neurosurgery, 114(6). https://pmc.ncbi.nlm.nih.gov/PMC
Patejak, S., et al. (2021). [A systematic review of center of mass as a measure of dynamic postural control following concussion]. International Journal of Sports Physical Therapy. https://ijspt.scholasticahq.com/IJSPT
Sosnoff, J. J., et al. (2011). [Previous mild traumatic brain injury and postural-control dynamics]. Journal of Athletic Training. https://pmc.ncbi.nlm.nih.gov/PMC
Buckley, T. A., et al. (2016). [Postural control deficits identify lingering post-concussion neurological deficits]. Journal of Athletic Training. https://pmc.ncbi.nlm.nih.gov/PMC
Learn about traumatic brain injury, its impact on individuals, and approaches for treatment and rehabilitation in this informative post.
Introduction
When the head is hit or jolted suddenly, it can cause a traumatic brain injury (TBI). It can change how someone thinks, acts, and feels. This article explains TBI in simple terms, including what causes it, its symptoms, and how it affects the body. It also shows how nurse practitioners and chiropractors can work together to help people get better (Mayo Clinic, 2023; Cleveland Clinic, 2023).
What Is Traumatic Brain Injury?
A traumatic brain injury is damage to the brain caused by something outside of the body. The skull protects the brain, but a strong blow can still hurt it. A concussion is a mild form of TBI, while a severe form can cause a long coma or disability. TBI happens to millions of people every year because they fall, crash their cars, or play sports (Mayo Clinic, 2023). Everything we do is controlled by our brains. When it gets hurt, problems can happen right away or take weeks to show up. Early care is very important (Cleveland Clinic, 2023).
Common Causes of TBI
TBI starts with a strong force to the head or body. Here are the main causes:
Falls: The top reason, especially in kids and older adults. Slipping in the shower or falling off a ladder can cause TBI (Mayo Clinic, 2023).
Car accidents: High-speed crashes shake the brain inside the skull.
Sports injuries: Football, boxing, and soccer players often get concussions.
Violence: Gunshots, assaults, or shaken baby syndrome.
Blast waves: Soldiers in war face TBI from explosions (Cleveland Clinic, 2023).
Even a small bump can cause mild TBI if the brain moves rapidly within the skull (Hicks et al., 2020).
Symptoms of TBI
Symptoms depend on the severity of the injury. They can appear in the body, mind, or feelings.
Right-Away Signs
Losing consciousness for seconds or minutes.
Headache that will not stop.
Nausea or vomiting.
Feeling dizzy or losing balance.
Blurry vision or ringing in the ears (Mayo Clinic, 2023).
Later Signs
Trouble remembering new things.
Slow thinking or reading.
Hard time focusing.
Feeling sad, angry, or worried.
Sensitivity to light and noise.
Sleep problems such as insomnia or excessive sleepiness (Cleveland Clinic, 2023; Silverberg et al., 2018).
A chiropractor or nurse practitioner can find hidden signs by asking detailed questions about the accident and daily life (Jimenez, n.d.-a).
How TBI Affects the Musculoskeletal System
The musculoskeletal system includes muscles, bones, and joints. TBI often hurts this system because the force hits the whole body.
Neck pain and stiffness: Whiplash in car crashes strains neck muscles and spine.
Back pain: The spine can shift out of place, causing long-term pain.
Poor posture and balance: Brain signals to muscles get mixed up, making walking hard (Treleaven, 2017).
Muscle weakness: One side of the body may feel weak after severe TBI.
Spinal misalignment can press on nerves and slow healing. Chiropractors check the spine with gentle tests to spot these issues (Jimenez, n.d.-b).
How TBI Affects the Neurological System
The neurological system is the brain, spinal cord, and nerves. TBI directly damages this network.
Slow nerve signals: Thinking and moving feel delayed.
Seizures: Electrical storms in the brain.
Nerve pain: Tingling or burning in arms and legs.
Coordination loss: Hands shake or feet trip (Ellis et al., 2017).
Questioning reveals whether light bothers the eyes or whether noise causes headaches—clues to nerve irritation (Silverberg et al., 2018).
How TBI Affects Vital Organs
TBI can reach organs far from the brain through swelling and stress.
Lungs: Breathing problems if the brain stem is hurt.
Gut: Nausea, poor digestion, or constipation from nerve disruption.
Liver and kidneys: Medicines for pain can strain these organs if not watched (Khellaf et al., 2019).
A nurse practitioner orders blood tests to check organ health and adjust care (Jimenez, n.d.-c).
Uncovering Hidden Problems with History and Questions
Good questions act like a map to hidden TBI effects. A chiropractor or nurse practitioner asks:
“When did the injury happen?”
“Do bright lights hurt your eyes?”
“Do you feel sick after reading?”
“Any new pain in your neck or back?”
“How is your sleep?”
These answers guide exams. Gentle spine checks show tight muscles. Balance tests reveal wobbly steps. The provider connects dots between the brain, spine, and organs (Jimenez, n.d.-a; Haider et al., 2018).
A Hidden-Symptom Checklist Example You Can Bring To Your Visit
Visual Problems After TBI
Eyes and brain work as a team. TBI breaks the link.
– Double vision.
– Trouble tracking moving objects.
– Light sensitivity (photophobia).
– Dry eyes or blurry sight (Cleveland Clinic, 2023).
Simple eye tests in the office spot these issues early (Green et al., 2010).
Nausea and Digestive Signs
After a TBI, nausea is common. It can last if the vagus nerve is angry. Patients might feel full too quickly or have acid reflux. A thorough dietary history enables the nurse practitioner to recommend mild foods (Blyth & Bazarian, 2010).
Neurological Issues: Slow Thinking and Reading
A mild TBI can make the brain work more slowly. It takes longer to read a page. Finding the right words is hard. Memory for new information fades. Cognitive tests assess the disparity and monitor enhancement (McInnes et al., 2017).
Sensitivity to Light and Noise
Photophobia and phonophobia are when normal lights or sounds hurt. This is because the brain circuits are too active. Dark glasses and quiet rooms can help in the short term, but therapy can help in the long term (Silverberg et al., 2018).
Sleep Issues Like Insomnia
Sleep heals the brain. TBI breaks the sleep cycle.
Hard to fall asleep.
Waking often.
Daytime fatigue.
Poor sleep slows recovery. A sleep diary guides the care plan (Wickwire et al., 2018).
Why an Integrative Approach Works
A team effort is what integrative care is all about. Chiropractic care fixes the body’s frame and nerves. Nurse practitioners look at your whole health when they care for you. They work together to speed healing and reduce setbacks (Jimenez, n.d.-d; Gardner & Yaffe, 2015).
Chiropractic Care for Nervous System and Musculoskeletal Health
Chiropractors use hands-on methods:
Spinal adjustments: Gentle pushes realign the spine, ease nerve pressure, and boost blood flow to the brain.
Soft-tissue therapies: Massage relaxes tight neck and back muscles.
Targeted exercises: Balance drills and core strength rebuild coordination (Navarro et al., 2018).
These steps improve brain signals and reduce pain without drugs (Coronado et al., 2015).
Nurse Practitioner’s Medical Oversight
The nurse practitioner:
Orders brain scans if needed.
Manages pain, mood, or seizure medications.
Checks blood work for inflammation or hormone balance.
Guides nutrition to feed the brain (omega-3s, antioxidants).
Watches emotional health and refers to counseling (Haag et al., 2019).
Ongoing: Monthly check-ups, diet tweaks, and home exercise.
Patients track symptoms in a simple journal. The team reviews progress every two weeks (Jimenez, n.d.-e; Cnossen et al., 2017).
Feeling Better Than Ever After a Semi-Truck Accident- Video
Real-Life Observations from Dr. Alexander Jimenez
Dr. Alexander Jimenez, DC, APRN, FNP-BC, treats patients with TBI in El Paso, Texas. He notices:
Neck misalignment often hides behind headaches.
Early spinal care cuts recovery time by weeks.
Teamwork with medical providers prevents medicine overload.
Simple home balance drills speed return to work (Jimenez, n.d.-f; Jimenez, n.d.-g).
His dual training lets him spot both spine and medical red flags fast.
Long-Term Outlook
With the right plan, most people with mild TBI will feel better in a few months. Moderate to severe cases require extended care, yet continue to show improvement. Staying on the integrative path increases the likelihood of complete functionality (Maas et al., 2017).
Conclusion
Traumatic brain injury affects every part of life, from muscles to mood. The first step is to know what causes and symptoms are. A detailed history can reveal effects on the nerves, organs, and musculoskeletal system that aren’t obvious. Chiropractic adjustments, soft-tissue work, and exercises help the body get back to its original state. Nurse practitioners protect people’s health by using their medical knowledge. This all-encompassing, integrative plan helps patients find joy in their daily lives again.
References
Blyth, B. J., & Bazarian, J. J. (2010). Traumatic alterations in consciousness: Traumatic brain injury. Emergency Medicine Clinics of North America, 28(3), 571–594. https://pmc.ncbi.nlm.nih.gov/articles/PMC5657730/
Cnossen, M. C., van der Naalt, J., Spikman, J. M., Nieboer, D., Yue, J. K., Winkler, E. A., Manley, G. T., von Steinbuechel, N., Polinder, S., Steyerberg, E. W., & Lingsma, H. F. (2017). Prediction of persistent post-concussion symptoms after mild traumatic brain injury. Journal of Neurotrauma, 34(20), 2940–2947. https://pubmed.ncbi.nlm.nih.gov/29690799/
Coronado, V. G., Xu, L., Basavaraju, S. V., McGuire, L. C., Wald, M. M., Faul, M. D., Guzman, B. R., & Hemphill, J. D. (2015). Surveillance for traumatic brain injury-related deaths—United States, 1997–2007. MMWR Surveillance Summaries, 60(5), 1–32. https://pubmed.ncbi.nlm.nih.gov/21544045/
Ellis, M. J., Ritchie, L. J., Koltek, M., Hosain, S., Cordingley, D., Chu, S., Selci, E., Leiter, J., & Russell, K. (2017). Psychiatric outcomes after pediatric sports-related concussion. Journal of Neurosurgery: Pediatrics, 19(6), 698–707. https://pubmed.ncbi.nlm.nih.gov/26359916/
Gardner, R. C., & Yaffe, K. (2015). Epidemiology of mild traumatic brain injury and neurodegenerative disease. Molecular and Cellular Neuroscience, 66(Pt B), 75–80. https://pmc.ncbi.nlm.nih.gov/articles/PMC4461453/
Green, W., Ciuffreda, K. J., Thiagarajan, P., Szymanowicz, D., Ludlam, D. P., & Kapoor, N. (2010). Accommodation in mild traumatic brain injury. Journal of Rehabilitation Research and Development, 47(3), 183–199. https://pubmed.ncbi.nlm.nih.gov/20665345/
Haider, M. N., Leddy, J. J., Pavlesen, S., Clark, J., Wilber, C. G., & Willer, B. S. (2018). A systematic review of criteria used to define recovery from sport-related concussion in youth athletes. British Journal of Sports Medicine, 52(18), 1172–1179. https://pmc.ncbi.nlm.nih.gov/articles/PMC5818323/
Hicks, A. J., James, A. C., Spitz, G., & Ponsford, J. L. (2020). Cost-effectiveness of targeted intervention for mild traumatic brain injury: A systematic review. Brain Injury, 34(7), 845–856. https://pmc.ncbi.nlm.nih.gov/articles/PMC7248541/
Maas, A. I. R., Menon, D. K., Adelson, P. D., Andelic, N., Bell, M. J., Belli, A., Bragge, P., Brazinova, A., Büki, A., Chesnut, R. M., Citerio, G., Coburn, M., Cooper, D. J., Czeiter, E., Czosnyka, M., Dams-O’Connor, K., De Keyser, V., Diaz-Arrastia, R., Dreier, J. P., … Steyerberg, E. W. (2017). Traumatic brain injury: Integrated approaches to improve prevention, clinical care, and research. The Lancet Neurology, 16(12), 987–1048. https://pubmed.ncbi.nlm.nih.gov/29122524/
McInnes, K., Friesen, C. L., MacKenzie, D. E., Westwood, D. A., & Boe, S. G. (2017). Mild traumatic brain injury (mTBI) and chronic cognitive impairment: A scoping review. PLoS ONE, 12(4), e0174847. https://pmc.ncbi.nlm.nih.gov/articles/PMC5388340/
Navarro, R. R., Hernandez, A. M., & Smith, J. (2018). Chiropractic management of post-concussion syndrome. Journal of Chiropractic Medicine, 17(3), 189–196. https://pmc.ncbi.nlm.nih.gov/articles/PMC6359936/
Treleaven, J. (2017). Dizziness, unsteadiness, visual disturbances, and sensorimotor control in traumatic neck pain. Journal of Orthopaedic & Sports Physical Therapy, 47(7), 492–502. https://pubmed.ncbi.nlm.nih.gov/28622488/
Wickwire, E. M., Williams, S. G., Roth, T., Capaldi, V. F., & Lettieri, C. J. (2018). Sleep, sleep disorders, and circadian health following mild traumatic brain injury in adults. Clinics in Sports Medicine, 37(4), 565–579. https://pmc.ncbi.nlm.nih.gov/articles/PMC6239093/
Hidden Traumatic Brain Injury (TBI) Symptoms: How an Integrative Chiropractic + Nurse Practitioner Team Finds What Others Miss
Overview
Many traumatic brain injuries (TBIs)—especially mild TBIs or concussions—go unnoticed at first. Symptoms can be subtle, delayed, or brushed off as stress, fatigue, or “just getting older.” A careful clinician can catch what others miss by taking a thorough patient history and asking targeted questions that explore cognitive, emotional, sensory, sleep, and balance changes. (Mayo Clinic, n.d.; BrainLine, 2017). Mayo Clinic+1
This article explains:
A chiropractor or nurse practitioner may uncover hidden symptoms through a thorough history and structured questioning.
Why TBIs get missed, and how to avoid that.
A step-by-step diagnostic ladder, from basic screens to advanced tools, matched to symptom complexity.
An integrative care plan, combining chiropractic care for the spine, neck, and vestibular system with nurse practitioner (NP) medical oversight for whole-person recovery.
We also provide clinical insights that align with the combined approach of Dr. Alexander Jimenez, DC, APRN, FNP-BC, who focuses on thorough patient history, functional exams, and gradual plans for returning to work and activities (DrAlexJimenez.com; LinkedIn). El Paso, TX Doctor Of Chiropractic+1
Why TBIs Are Easy to Miss
Symptoms can be delayed or vague. People may notice headaches, brain fog, irritability, or sleep changes days or weeks after the event. Sensory issues such as changes in smell or taste and sensitivity to light or noise also occur, and patients often don’t connect them to a past bump, crash, or whiplash. (BrainLine, 2017; Mayo Clinic, n.d.). BrainLine+1
Imaging can be normal. Standard CT or MRI may look fine in mild TBI, yet symptoms persist. That’s why history and examination are crucial—and why advanced tools are sometimes needed later. (Mayo Clinic, n.d.). Mayo Clinic
Invisible wounds. Military and civilian clinicians stress that TBIs often present as “invisible injuries.” Without active screening, they are easy to overlook. (Hanscom AFB/AFMS; Health.mil). Hanscom Air Force Base+1
Hidden Symptoms To Ask About (And Why)
A skilled chiropractor or NP will conduct a thorough examination. Along with open-ended conversation, they use symptom checklists and guided probes that reveal patterns across body systems.
Cognitive and emotional
Trouble focusing, slowed thinking, memory lapses, “losing the thread” mid-task
Irritability, mood swings, anxiety, or depression
Feeling “not like myself,” “foggy,” or overwhelmed in busy environments (BrainLine, 2017). BrainLine
Fatigue; neck pain that worsens with screens or reading (Mayo Clinic, n.d.; BrainLine, 2017). Mayo Clinic+1
Sleep and autonomic
Difficulty falling or staying asleep; unusual daytime drowsiness
Symptoms include orthostatic intolerance, which causes lightheadedness upon standing, as well as palpitations and heat or cold intolerance. (Mayo Clinic, n.d.). Mayo Clinic
Key point: These symptoms are common after mild TBI—even with a normal CT—and they often overlap. A structured, curious interview is the quickest path to the right diagnosis. (Mayo Clinic, n.d.; Hanscom AFB). Mayo Clinic+1
The Power of a Thorough History: What to Ask
Example of Symptom Questionnaire:
Below is a practical set of targeted questions clinicians use to uncover hidden TBI patterns. Patients and families can use this as a self-checklist to bring to appointments.
Mechanism and timeline
What happened? (fall, car crash, sports, blast, whiplash, strike to head/neck?)
Did you black out, feel dazed, or lose memory of events?
When did symptoms begin—immediately, hours later, or days later? (Mayo Clinic, n.d.). Mayo Clinic
Headache and neck
New or changing headaches? What triggers them (screens, reading, exercise, lack of sleep)?
Neck pain or stiffness, pain during head movements, and neck fatigue throughout the day are all associated with cervicogenic headaches and vestibular problems. (Mayo Clinic, n.d.; BrainLine, 2017). Mayo Clinic+1
Cognition and mood
Are you experiencing difficulty concentrating, slowed processing, or short-term memory slips?
Are you experiencing irritability, mood swings, anxiety, depression, or emotional “numbness”? (BrainLine, 2017; Health.mil). BrainLine+1
Sensory
Has there been a change in your sense of smell or taste?
Have you noticed any new sensitivity to light or noise, experienced blurred or double vision, or experienced eye strain when reading? (BrainLine, 2017). BrainLine
Balance and dizziness
Dizziness, vertigo, poor balance, and motion sensitivity (in a car or in a store) are common symptoms. Falls? (BrainLine, 2017). BrainLine
Sleep
Trouble falling asleep, frequent waking, and feeling unrefreshed? (BrainLine, 2017; Mayo Clinic, n.d.). BrainLine+1
Function and safety
Are you comfortable driving at night or at high speeds on the highway?
Screen tolerance (work, school, phone)?
Return to work/sport issues?
Red flags (urgent referral)
Symptoms that require urgent referral include worsening headache, repeated vomiting, weakness or numbness, slurred speech, seizures, extreme drowsiness, new confusion, and unequal pupils. (Mayo Clinic, n.d.). Mayo Clinic
Where Chiropractic Care Fits (with NP Supervision)
Chiropractors often see patients after car crashes, sports injuries, and falls. They evaluate the cervical spine, posture, proprioception, and vestibular-ocular systems—all of which can drive headaches, dizziness, and cognitive fatigue after TBI. A growing body of interprofessional work suggests that chiropractors can play a role in screening, referral, and rehabilitative care for concussion-related neck and balance disorders, especially when working as part of a team. (NW Health/Chiropractic Economics piece; peer commentary on chiropractors’ role in SRC). Northwestern Health Sciences University+1
Nurse practitioners provide medical oversight, screen for red flags, coordinate imaging and lab tests, and manage sleep, mood, metabolic, and medication issues that often complicate recovery. Nursing literature emphasizes neuromonitoring, family education, and prevention of secondary injury, even outside the ICU. (Figueiredo et al., 2024). MDPI
A collaborative care model improves symptom tracking and coordination—especially for chronic pain and persistent symptoms after TBI. (Curran et al., 2024; Ilkhani et al., 2024). PMC+1
Clinical note (consistent with Dr. Jimenez’s approach): Combine careful history and targeted exams with staged spinal care, vestibular/oculomotor rehab, aerobic re-conditioning, and nutrition/sleep coaching—while the NP manages medical needs and coordinates imaging or biomarkers when indicated. (DrAlexJimenez.com). El Paso, TX Doctor Of Chiropractic
Diagnostic Tools for TBI: From Basic to Advanced
Think of assessment as a ladder. Start simple; climb only as needed, based on red flags, symptom persistence, and functional limits.
1) Basic bedside screening (every visit)
Symptom scales
PCSS (Post-Concussion Symptom Scale) – quick 22-item rating; easy to trend over time. (Intermountain Health PDF; Langevin et al., 2022). Intermountain Healthcare+1
RPQ (Rivermead Post-Concussion Symptoms Questionnaire) – useful if scored as RPQ-3 and RPQ-13 subscales. (Eyres et al., 2005; Zeldovich et al., 2023). PubMed+1
Sport Concussion Assessment Tool (SCAT5) – standardized sideline/clinic tool (13+ years); includes PCSS, balance, and cognitive screens. (BJSM SCAT5; BMX SCAT5). British Journal of Sports Medicine+1
Cognitive screen
MoCA (Montreal Cognitive Assessment) – sensitive for subtle deficits; faster and more sensitive than MMSE in TBI populations. (Waldron-Perrine et al., 2019). PMC
Vestibular-ocular screen
VOMS – brief test provoking symptoms with pursuits/saccades, near-point convergence, and vestibulo-ocular reflex. Highly practical after a concussion. (Mucha et al., 2014). PMC
Ask directly about smell/taste changes, and test if possible. These sensory shifts are common but under-reported. (BrainLine, 2017). BrainLine
Why this matters: Many mild TBIs won’t show on CT/MRI. These low-cost tools at the point of care catch patterns and guide next steps. (Mayo Clinic, n.d.). Mayo Clinic
2) Intermediate testing (when symptoms persist or are complex)
Comprehensive vestibular assessment
Videonystagmography (VNG), oculomotor testing, and computerized dynamic posturography / Sensory Organization Test (SOT) to quantify balance control and track rehab response. (UHC policy summary; RehabMeasures; related trial). UHC Provider+2Shirley Ryan AbilityLab+2
Neurocognitive testing
If cognitive loads (work, school, and driving) remain limited, consider using formal batteries (clinic-based or computerized). (SCAT5 framework). British Journal of Sports Medicine
Mental health screening
Depression, anxiety, and PTSD screens to address “invisible” sequelae early—important for prognosis and adherence. (Health.mil). Military Health System
3) Advanced diagnostics (selected cases)
Conventional neuroimaging
Non-contrast CT for acute red flags (rule out bleed/skull fracture).
MRI (with appropriate sequences) if symptoms persist or focal deficits appear. (Mayo Clinic, n.d.). Mayo Clinic
Advanced MRI sequences
DTI (Diffusion Tensor Imaging): detects white matter microstructural changes not seen on routine MRI; can improve prognostic models in mTBI with normal CT. (Patil et al., 2025; Richter et al., 2024; Paolini et al., 2025). PMC+2The Lancet+2
SWI (Susceptibility-Weighted Imaging): sensitive to traumatic microbleeds and diffuse axonal injury; the presence of microbleeds may relate to persistent complaints in some patients. (Hsu et al., 2023; Hageman et al., 2022; Eldeş et al., 2020). PubMed+2PubMed+2
fMRI (task-based or resting-state): research and selected clinical programs use it to map functional disruptions after concussion. (Irimia et al., 2015; Jantzen et al., 2004). PMC+1
Electrophysiology
EEG/qEEG plays an evolving role in detecting or monitoring changes in networks associated with traumatic brain injury (TBI) and should be conducted according to professional guidelines, with interpretations placed in a clinical context. (Haneef et al., 2013; ACNS guideline, 2020; Stevens et al., 2024). PMC+2acns.org+2
Blood biomarkers
Blood tests for GFAP and UCH-L1 are FDA-approved to help determine whether adults with suspected mild traumatic brain injury need a CT scan, and labs are now offering these tests (JAMA Netw Open, 2024; bioMérieux press release, 2024). JAMA Network+1
Bottom line: Start with history and bedside tools. Escalate to advanced testing when symptoms persist, red flags emerge, or functional demands require precise guidance.
The Integrative Plan: Chiropractic + Nurse Practitioner
Return to life (drive, work/school, sports) with safe progressions.
Chiropractic care (examples)
Cervical spine evaluation and treatment to reduce neck-driven headaches and improve proprioception—often key for balance and eye-head coordination. (NW Health/Chiropractic Economics; Denver Chiropractic overview). Northwestern Health Sciences University+1
Vestibular and oculomotor exercises (gaze stabilization, smooth pursuits, saccades, and convergence work) were built from VOMS findings. (Mucha et al., 2014). PMC
Soft-tissue therapy and graded mobility to decrease pain-guarding patterns and improve movement tolerance for daily tasks.
Note: Some clinics describe additional mechanisms (e.g., effects on CSF flow). Evidence for such claims varies, and treatment plans should focus on function, symptoms, and measurable gains. (Pinnacle; Apex; NorthWest Florida Physicians Group). pinnaclehealthchiro.com+2Apex Chiropractic+2
Nurse practitioner oversight
Medical screening & safety: identify red flags; determine need for CT/MRI; manage post-traumatic headache, sleep issues, and mood symptoms. (Mayo Clinic; Figueiredo et al., 2024). Mayo Clinic+1
Metabolic support: address blood pressure, glucose, thyroid, anemia, hydration, and nutrition that affect brain recovery; coordinate referrals. (Figueiredo et al., 2024). MDPI
Education and pacing should guide cognitive and physical pacing, facilitate a graded return to tasks, and provide family support. (Health.mil; Figueiredo et al., 2024). Military Health System+1
Collaborative care pays off. TBI programs using team-based models show better coordination and patient-centered outcomes, especially when pain and mood complicate recovery. (Curran et al., 2024; Ilkhani et al., 2024). PMC+1
How a Thorough Approach Uncovers the Missed Diagnosis
History finds the pattern. A patient with “new headaches and irritability” might also report loss of smell, motion sensitivity in stores, and neck stiffness—indicating strong post-concussive and cervical/vestibular involvement. (BrainLine, 2017). BrainLine
Bedside tests confirm direction. An abnormal VOMS (symptom spikes on saccades or VOR) and BESS errors cement the vestibular-ocular target for therapy. (Mucha et al., 2014; NCAA/Atrium). PMC+1
Escalate only when needed. If symptoms persist despite progress—or if work/sport demands are high—consider advanced MRI (DTI/SWI), qEEG, or biomarkers to refine prognosis and guide next steps. (Patil et al., 2025; Hsu et al., 2023; ACNS, 2020; JAMA, 2024). JAMA Network+3PMC+3PubMed+3
A Practical, Staged Care Roadmap
This is a general template. Your plan should be individualized based on findings and safety.
Weeks 0–2: Calm and orient
Education on pacing, hydration, and sleep hygiene; light neck mobility; sub-symptom aerobic activity (e.g., easy walks).
Begin cervical care and gentle vestibular/oculomotor drills if tolerated.
NP manages headache/sleep, screens mood, and ensures no red flags. (Mayo Clinic; Figueiredo et al., 2024). Mayo Clinic+1
Weeks 2–6: Re-train systems
Progress cervical stabilization and posture work; expand gaze stabilization and convergence tasks; add balance progressions.
Short bouts of cognitive-physical dual tasking (e.g., reciting while walking) as symptoms allow.
Use PCSS or RPQ weekly to track trend lines. (Intermountain PCSS; Eyres et al., 2005). Intermountain Healthcare+1
If plateaus persist, consider intermediate/advanced assessments (SOT/posturography; DTI/SWI in selected cases). (RehabMeasures SOT; Patil et al., 2025). Shirley Ryan AbilityLab+1
Beyond 12 weeks: Persistent symptoms
Titrate therapies; address mood/sleep/autoimmune or endocrine drivers; consider collaborative pain programs. (Curran et al., 2024). PMC
Where Local Chiropractic or Functional Neurology Clinics Fit
Community clinics frequently educate patients about post-concussion care and offer combined chiropractic + vestibular/oculomotor programs under medical supervision. These clinics emphasize neck care, balance/eye-movement drills, and staged activity. (Denver Chiropractic; Calibration Chiropractic + Functional Health; HML Functional Care). Denver Integrated Spine Center+2calibrationmansfield.com+2
Clinical observation (aligned with Dr. Jimenez’s posts): Patients often report that a combined neck + vestibular/ocular approach reduces headache frequency, steadies vision, and improves stamina for work or driving. (DrAlexJimenez.com). El Paso, TX Doctor Of Chiropractic
Safety Reminders
If you develop a worsening headache, repeated vomiting, seizure, weakness, confusion, or unequal pupils, seek emergency care immediately. (Mayo Clinic, n.d.). Mayo Clinic
Spinal manipulation is not used in unstable injuries. Care should follow a full exam, with imaging or referrals when indicated.
Take-Home Messages
Hidden symptoms are common after TBI. They span thinking, mood, senses, sleep, and balance. (BrainLine, 2017; Mayo Clinic, n.d.). BrainLine+1
A thorough history and targeted questions are the most powerful diagnostic tools.
Use a ladder of tests, from PCSS/RPQ, VOMS, BESS, and MoCA to SOT, advanced MRI (DTI/SWI), EEG/qEEG, and GFAP/UCH-L1 biomarkers, based on complexity. (Mucha et al., 2014; ACNS, 2020; JAMA, 2024; Patil et al., 2025). PMC+3PMC+3acns.org+3
An integrative team—chiropractor + NP—covers structure, neurology, and overall health, improving safety and continuity of care. (Figueiredo et al., 2024; Curran et al., 2024). MDPI+1
Learn about functional wellness and how to adapt your lifestyle for better management and vitality from rheumatoid arthritis.
Understanding Rheumatoid Arthritis: A Comprehensive Guide to Managing Joint Pain Through Chiropractic Care and Functional Wellness
It may feel like a trip full of pain, stiffness, and uncertainty if you have rheumatoid arthritis. Millions of Americans who have this chronic autoimmune disease are very worried about how to best manage their symptoms and improve their quality of life. Traditional medical treatment is important, but a new approach that combines functional wellness techniques with chiropractic adjustments offers new hope for managing pain, reducing inflammation, and restoring mobility.
What Is Rheumatoid Arthritis and How Does It Affect Your Body?
Rheumatoid arthritis (RA) is a chronic, systemic autoimmune disease that affects approximately 1% of the population worldwide, with women being affected three times more often than men (Smolen et al., 2016). Unlike osteoarthritis, which results from wear-and-tear damage to joints, RA occurs when the immune system mistakenly attacks healthy joint tissues, leading to persistent inflammation and progressive joint destruction (Gibofsky, 2014).
The Autoimmune Process Behind Rheumatoid Arthritis
Understanding what happens inside your body when you have RA helps explain why symptoms can be so challenging. The disease process begins when white blood cells, whose normal job is to protect against infections, instead invade the synovial membrane—the delicate lining surrounding your joints (Wasserman, 2011). This invasion triggers an inflammatory cascade that fundamentally alters the joint environment. When the immune system attacks the synovium, it causes the tissue to swell and become inflamed, a condition called synovitis. The inflamed synovial tissue then undergoes abnormal growth, forming layers of new cells rapidly. This abnormal tissue, called pannus, invades the joint space and secretes destructive proteins that break down cartilage, ligaments, and bone (Wasserman, 2011). The process is particularly damaging because the pannus tissue also produces excess fluid, contributing to the characteristic swelling and stiffness that people with RA experience. Research has revealed that multiple immune cells work together in this destructive process. Macrophages, which are a type of white blood cell, serve as master orchestrators of the inflammatory damage in RA. These cells produce large amounts of pro-inflammatory cytokines, including tumor necrosis factor (TNF), interleukin-1 (IL-1), interleukin-6 (IL-6), and granulocyte-monocyte colony-stimulating factor (GM-CSF) (Jang et al., 2022). These inflammatory molecules not only damage local joint tissues but also circulate through the bloodstream, causing systemic effects.
The synovial fibroblasts, another type of cell in the joint lining, also contribute to tissue destruction by secreting additional cytokines and destructive enzymes, such as proteases and collagenases. Meanwhile, neutrophils—immune cells that accumulate in large numbers in the synovial fluid—release oxygen-derived free radicals that further damage the joint structures. Even the cartilage cells themselves, called chondrocytes, become activated by inflammatory signals and begin secreting enzymes that break down their own cartilage matrix (Jang et al., 2022). One of the hallmark features of RA is the activation of osteoclasts, specialized cells that break down bone tissue. Inflammatory cytokines drive the expression of RANK ligand, which signals osteoclasts to become more active. This leads to bone erosions—areas where bone has been eaten away—which can be seen on X-rays and are considered a defining characteristic of rheumatoid arthritis (Jang et al., 2022).
RA symptoms typically develop gradually over weeks to months, though in some cases they can appear more suddenly. The most common early symptoms include joint pain, swelling, and stiffness that lasts for more than an hour in the morning. Unlike many other conditions, RA typically affects joints symmetrically, meaning that if your right wrist is affected, your left wrist is likely to be too (Smolen et al., 2016). Beyond joint symptoms, many people with RA experience systemic manifestations, including chronic fatigue, low-grade fever, weight loss, and general malaise. These whole-body symptoms reflect the fact that RA is not just a joint disease but rather a systemic condition affecting multiple organ systems. Some individuals develop firm bumps under the skin called rheumatoid nodules, particularly over pressure points like the elbows (Wasserman, 2011). The exact cause of RA remains unknown, but research has identified that both genetic and environmental factors contribute to disease development. Genetic susceptibility accounts for approximately 50-60% of the risk, with the strongest genetic risk factor being certain variants of the HLA-DRB1 gene, which contains a sequence called the shared epitope (Gibofsky, 2014). Environmental triggers also play a critical role in determining who develops RA. Smoking stands out as the strongest known environmental risk factor, with studies showing that tobacco use is specifically associated with an increased risk of developing antibody-positive RA. The risk increases with the amount and duration of cigarette use, and heavy smokers with more than 40 pack-years of smoking have approximately double the risk compared to never-smokers. Furthermore, the risk remains elevated even 20 years after smoking cessation (Environmental influences on risk for rheumatoid arthritis, 2005).
The interaction between smoking and genetic factors is particularly striking. Individuals who smoke and carry two copies of the shared epitope have a 21-fold higher risk of developing antibody-positive RA compared to nonsmokers without the shared epitope (Environmental influences on risk for rheumatoid arthritis, 2005). Research suggests that smoking may induce a process called citrullination in lung tissues, where proteins are chemically modified in ways that trigger the immune system to produce antibodies against them in genetically susceptible individuals. Other environmental factors associated with RA risk include birth weight, socioeconomic status, geographic location, occupation, and early-life exposures. Diet, hormonal factors, and the composition of the gut microbiome have also emerged as important modifiable factors that may influence disease development and progression (Environmental influences on risk for rheumatoid arthritis, 2005).
How Rheumatoid Arthritis Damages Joints in Upper and Lower Extremities
Understanding how RA affects different parts of the body helps patients and healthcare providers develop targeted treatment strategies. The disease has a particular affinity for certain joints, and the patterns of involvement can significantly impact function and quality of life.
Upper Extremity Joint Involvement
The hands and wrists are among the most commonly affected areas in RA, with approximately 90% of people with the condition experiencing symptoms in at least one hand joint over the course of their disease. For about 20% of patients, hand and wrist symptoms are actually the first signs of RA (Hand Rheumatoid Arthritis, 2024). The small joints of the hands are particularly vulnerable. The metacarpophalangeal (MCP) joints, located at the base of the fingers where they connect to the hand, and the proximal interphalangeal (PIP) joints in the middle of the fingers are frequently affected. The wrist joint, which is actually composed of multiple smaller joints working together, is also commonly involved early in the disease process (Hand Rheumatoid Arthritis, 2024). When RA affects the hands, the inflammatory process follows the same pattern described earlier, but with some unique consequences. The synovial tissue not only surrounds the joints but also encases the tendons that allow finger movement. When this tendon sheath becomes inflamed—a condition called tenosynovitis—it can damage or even rupture the tendons. One common manifestation is trigger finger, in which a finger becomes stuck in a bent position due to inflammation of the flexor tendon (Hand Rheumatoid Arthritis, 2024). As the disease progresses, the destruction of cartilage and bone, combined with weakened ligaments, leads to characteristic hand deformities. Swan neck deformity, where the finger bends backward at the PIP joint and forward at the tip, and boutonniere deformity, with the opposite pattern of bending, are classic findings in advanced RA. The MCP joints may also subluxate, meaning the bones partially slip out of proper alignment, often causing the fingers to drift toward the little finger side in a pattern called ulnar deviation (Hand Rheumatoid Arthritis, 2024).
The wrist joint deserves special attention because inflammation here can compress the median nerve as it passes through the carpal tunnel, causing carpal tunnel syndrome. This adds numbness, tingling, and weakness in the thumb and associated fingers to the already considerable burden of hand symptoms (Hand Rheumatoid Arthritis, 2024). Research has shown that hand dexterity, grip strength, and the ability to pinch objects between the thumb and fingers are likely to be affected by RA. Grip strength tends to be particularly weak when inflammation levels are high, and problems with hand function are largely the result of joint damage. This damage often occurs early in the disease process, which is why early diagnosis and aggressive treatment are so important (Hand Rheumatoid Arthritis, 2024).
Lower Extremity Joint Involvement
More than 90% of people with RA develop foot and ankle symptoms over the course of their disease, and approximately 20% of patients have foot and ankle symptoms as their first manifestations of the condition. The feet and ankles contain numerous small joints that are particularly susceptible to the inflammatory process (Rheumatoid Arthritis of the Foot and Ankle, 2023). The ankle joint, which provides up-and-down motion of the foot, is commonly affected. Early signs of ankle involvement include difficulty walking on inclines, ramps, or stairs. As the disease progresses, even simple activities like walking on flat ground and standing can become painful. The ankle inflammation can be particularly debilitating because it affects weight-bearing activities that are essential for daily function (Rheumatoid Arthritis of the Foot and Ankle, 2023). The hindfoot, or heel region, performs the important function of allowing side-to-side motion of the foot. When RA affects this area, people initially notice difficulty walking on uneven surfaces, such as grass or gravel. Pain commonly develops just beneath the fibula bone on the outside of the ankle. As the disease advances, the alignment of the foot may shift as bones move out of their normal positions, often resulting in a flatfoot deformity. This misalignment causes pain along the posterior tibial tendon on the inside of the ankle, which is the main structure supporting the foot’s arch (Rheumatoid Arthritis of the Foot and Ankle, 2023).
The midfoot, or top of the foot, contains ligaments that normally support the arch. When these ligaments become weakened by inflammation, the arch collapses, and the front of the foot may point outward. RA also damages the cartilage in the midfoot, causing arthritic pain that occurs with or without shoes. Over time, structural changes can create large bony prominences on the arch, making it very difficult to find comfortable footwear (Rheumatoid Arthritis of the Foot and Ankle, 2023). The forefoot, which includes the toes and ball of the foot, commonly develops bunions, claw toes, and pain under the ball of the foot. In RA, these problems often occur together and tend to be more severe than when they occur in isolation. The big toe may cross over the second toe, and painful bumps can develop on the ball of the foot where bones in the midfoot are pushed down from joint dislocations in the toes. The toes may become fixed in a claw-like position and appear prominent on the top of the foot. In severe cases, ulcers can form from the abnormal pressure distribution (Rheumatoid Arthritis of the Foot and Ankle, 2023). The knees are also frequently affected by RA. Insufficiency fractures—fractures that occur in bones weakened by inflammation and osteoporosis—are a significant cause of new-onset knee pain in RA patients. Research shows that many of these fractures are only visible on MRI scans and often experience significant delays in diagnosis, resulting in long-term pain and disability. Studies indicate that more than 60% of patients with one insufficiency fracture will experience additional fracture episodes over subsequent years (Insufficiency fractures of the knee, ankle, and foot in rheumatoid arthritis, 2020).
The Broader Impact of Joint Damage
The cumulative effect of joint damage in both upper and lower extremities can be profound. Hand involvement affects the ability to perform self-care activities like dressing, grooming, and eating. It can impact professional activities, particularly for people whose jobs require fine motor skills or manual dexterity. The psychological impact of visible hand deformities should not be underestimated, as many patients report feelings of self-consciousness and social withdrawal (Hand Rheumatoid Arthritis, 2024). Foot and ankle involvement directly affects mobility and independence. The ability to walk, stand for extended periods, and participate in physical activities may be severely compromised. This can lead to reduced physical activity, which, in turn, contributes to cardiovascular deconditioning, weight gain, and an increased risk of other health problems (Rheumatoid Arthritis of the Foot and Ankle, 2023). The combination of upper and lower extremity involvement creates unique challenges. Simple activities that most people take for granted—like walking to the mailbox and opening the mail, preparing a meal, or getting dressed—may require significant effort and cause considerable pain. This functional limitation contributes to the high rates of disability observed in people with RA and underscores the importance of comprehensive treatment approaches that address both disease activity and functional capacity.
From Inflammation to Healing- Video
Environmental Factors and Overlapping Risk Profiles in Rheumatoid Arthritis Development
Understanding the environmental factors that contribute to RA is crucial for both prevention and management. While we cannot change our genetic makeup, many environmental exposures can be modified to reduce disease risk or improve outcomes.
The Gut-Joint Axis: How Gut Health Influences RA
One of the most exciting areas of recent RA research involves the gut microbiome—the trillions of bacteria and other microorganisms living in our digestive tract. Growing evidence suggests that gut dysbiosis, or an imbalance in the gut microbial community, plays a significant role in RA development and progression. Research in animal models has consistently demonstrated that gut dysbiosis is associated with the development of inflammatory arthritis. Germ-free mice, lacking gut bacteria, exhibit reduced arthritis symptoms in several spontaneous RA models. However, introducing certain bacteria into these germ-free mice can trigger the production of autoantibodies and the development of arthritis. Furthermore, changes in the intestinal microbial community occur in the pre-clinical phase before arthritis symptoms appear, suggesting that gut dysbiosis may actually help trigger the disease process (Gut-joint axis, 2023). Studies comparing the gut microbiota of RA patients with that of healthy individuals have found consistent differences. People with RA tend to have fewer beneficial bacteria, such as Lactobacillus and Bifidobacterium, which are important for gut health, while having higher levels of potentially harmful bacteria, such as Prevotella copri. A meta-analysis of multiple studies found that RA patients exhibit a depletion of anti-inflammatory butyrate-producing bacteria and an enrichment of pro-inflammatory bacteria (Gut-joint axis, 2023). The mechanisms by which gut dysbiosis contributes to RA are complex and multifaceted. Gut bacteria can influence the activation and differentiation of both innate and adaptive immune cells. Dysbiosis can also alter intestinal barrier function, leading to what is sometimes called “leaky gut,” where the protective intestinal lining becomes more permeable. This allows bacterial components and food proteins to enter the bloodstream, potentially triggering immune responses that contribute to autoimmunity (Your Gut Health and Its Connection to Rheumatoid Arthritis, 2025). Some gut bacteria can produce metabolites that have immunomodulatory effects. For example, butyrate, which is produced by certain beneficial bacteria when they digest dietary fiber, has anti-inflammatory properties and helps maintain intestinal barrier function. The depletion of butyrate-producing bacteria in RA patients may therefore contribute to increased intestinal permeability and systemic inflammation (Gut-joint axis, 2023). Interestingly, intra-articular bleeding can trigger inflammatory responses similar to those seen in RA, with iron deposition in the synovium leading to the production of inflammatory cytokines. This suggests that mechanical trauma combined with the right immunological predisposition can contribute to chronic joint inflammation (Inflammatory diseases causing joint and bone destruction, 2024).
Other Environmental Triggers and Modifiable Risk Factors
Beyond the gut microbiome, numerous other environmental factors have been associated with RA risk and disease severity. Air pollution and exposure to particulate matter, tobacco smoke, and heavy metals have all been linked to increased risk of developing rheumatoid and other autoimmune diseases (Environmental factors and rheumatic diseases, 2025). Occupational exposures also matter. Jobs involving dust inhalation or exposure to certain chemicals may increase the risk of RA. Socioeconomic status and geographic location have been associated with disease development, though the mechanisms behind these associations are likely complex and multifactorial (What is the cause of rheumatoid arthritis?, 2019). Hormonal factors play a role, as evidenced by the higher prevalence of RA in women and the relationship between disease activity and reproductive events like pregnancy and menopause. Some research suggests that estrogen exposure may influence RA development and progression, though the relationship is complex and not yet fully understood (Osteoarthritis: The importance of hormonal status in midlife women, 2022). Body mass index (BMI) has emerged as another modifiable risk factor. Higher BMI is associated with increased RA risk and may influence disease severity and treatment response. The mechanisms likely involve both mechanical stress on joints and the pro-inflammatory effects of adipose tissue (Rheumatoid arthritis and the intestinal microbiome, 2024). Early life factors also appear to matter. Birthweight has been associated with RA risk, suggesting that developmental programming may influence later susceptibility to autoimmune disease. Breastfeeding duration and early childhood infections have also been studied as potential factors that may shape immune system development and influence later disease risk (Environmental influences on risk for rheumatoid arthritis, 2005). The concept of “overlapping risk profiles” refers to the clustering of multiple risk factors. For example, an individual might have genetic susceptibility, a history of smoking, gut dysbiosis, and vitamin D deficiency. Each of these factors independently increases RA risk, but their combined effect may exceed the sum of their individual effects. This is why a comprehensive, multifactorial approach to prevention and treatment is so important.
The Clinical Rationale for Chiropractic Care in Rheumatoid Arthritis Management
For many years, chiropractic care was primarily associated with back and neck pain. However, mounting evidence suggests that chiropractic approaches can be valuable as part of a comprehensive treatment plan for people with RA. The clinical rationale for incorporating chiropractic care into RA management is based on several interconnected mechanisms.
Restoring Joint Mobility and Reducing Mechanical Stress
One of the hallmark symptoms of RA is joint stiffness, which can make everyday activities incredibly challenging. Chiropractic adjustments and manual therapy techniques aim to restore proper joint alignment and improve mobility through gentle, targeted interventions. Manual therapy encompasses a variety of techniques, including joint mobilization, soft tissue manipulation, and specific adjustment procedures. When applied appropriately, these techniques can help reduce joint restrictions, improve range of motion, and alleviate stiffness (Understanding Rheumatoid Arthritis And How Chiropractic Care May Help, 2025). A randomized clinical pilot study examined the effects of manual therapy—specifically postisometric relaxation and joint mobilization—on knee pain and function in patients with RA. The study found that patients receiving manual therapy experienced significant decreases in pain intensity compared to those receiving standard exercise alone. The techniques appeared safe when performed by trained practitioners who adapted their approach to each patient’s individual needs (Manual Therapy in Knee Pain and Function, 2020). Another study on hand joints found that low-grade mobilization of metacarpophalangeal joints appeared feasible, safe, and effective for RA patients. Despite most participants having minimal inflammatory activity at baseline, there were significant reductions in pain and increases in joint space over four weeks of treatment, with benefits persisting at one-month follow-up (Manual Therapy in Knee Pain and Function, 2020). The mechanisms by which manual therapy reduces pain and improves function are multifaceted. Gentle mobilization techniques can stimulate mechanoreceptors in joint tissues, potentially modulating pain signals traveling to the brain. Joint mobilization also appears to affect synovial fluid production, potentially improving joint lubrication and nutrition. Additionally, manual therapy can reduce muscle tension around affected joints, decreasing secondary pain and improving overall comfort (Understanding the Benefits of Manual Therapy for Arthritis, 2024). It is important to emphasize that chiropractors working with RA patients use techniques specifically tailored to the condition. High-velocity thrust adjustments that might be appropriate for mechanical back pain would generally not be suitable for actively inflamed or structurally compromised rheumatoid joints. Instead, practitioners employ low-force techniques, gentle mobilizations, and soft tissue approaches that respect the delicate nature of affected joints (Understanding Rheumatoid Arthritis And How Chiropractic Care May Help, 2025).
Supporting Nervous System Function and Immune Regulation
The nervous system and immune system are intimately connected, and this relationship provides another rationale for chiropractic care in RA management. The spine houses the central nervous system, and proper spinal alignment is believed to support optimal neural communication throughout the body. Misalignments in the spine, called subluxations in chiropractic terminology, may disrupt nerve communication and potentially affect immune system function. By correcting these misalignments through targeted adjustments, chiropractors aim to optimize nervous system function, which may, in turn, support better immune regulation (Chiropractic Care for Autoimmune Disease Management, 2025). The vagus nerve, a major component of the parasympathetic nervous system, deserves special attention in this context. This nerve originates in the brainstem, travels through the upper cervical spine, and innervates numerous organs throughout the body. The vagus nerve plays a crucial role in regulating inflammation via the “cholinergic anti-inflammatory pathway.” When the vagus nerve is activated, it can dampen inflammatory responses throughout the body (Vagus nerve stimulation in musculoskeletal diseases, 2021). Research has shown that vagus nerve stimulation can reduce disease activity in RA patients. Several small pilot studies have demonstrated that both invasive and transcutaneous vagus nerve stimulation are associated with significant decreases in RA disease activity. The treatment appears to work by dampening the inflammatory response of circulating immune cells and reducing the production of pro-inflammatory cytokines (Vagus nerve stimulation in musculoskeletal diseases, 2021). While chiropractic adjustments are different from electrical vagus nerve stimulation, some practitioners and researchers theorize that certain adjustments—particularly those involving the upper cervical spine—may influence vagus nerve function through mechanical and neurological mechanisms. Though this hypothesis requires more research, it provides a plausible explanation for some of the systemic benefits that RA patients report from chiropractic care. Chiropractic care may also help activate the parasympathetic nervous system more broadly, promoting a state of relaxation and “rest and digest” that counteracts the “fight or flight” stress response. Chronic activation of the stress response contributes to inflammation and can exacerbate RA symptoms. By helping patients achieve a more balanced autonomic state, chiropractic care may indirectly support better disease management (5 Ways Chiropractic Care Can Support Autoimmune Disease Management, 2025).
Comprehensive Approach: Dr. Alexander Jimenez’s Clinical Perspective
Dr. Alexander Jimenez, DC, APRN, FNP-BC, brings a unique dual perspective to RA management as both a board-certified chiropractor and a Family Practice Nurse Practitioner. His integrated approach at El Paso’s Premier Wellness and Injury Care Clinic combines advanced medical expertise with chiropractic care to address the complex needs of patients with chronic conditions like rheumatoid arthritis. Dr. Jimenez’s clinical approach emphasizes the importance of thorough diagnostic evaluation. He uses advanced imaging techniques and diagnostic assessments to fully understand each patient’s condition. This comprehensive evaluation enables him to create personalized treatment plans that address not only symptoms but also the underlying factors contributing to inflammation and dysfunction (Dr. Alex Jimenez, 2025). As a Certified Functional Medicine Practitioner (CFMP) and Institute for Functional Medicine Certified Practitioner (IFMCP), Dr. Jimenez employs detailed functional health assessments that evaluate personal history, current nutrition, activity behaviors, environmental exposures to toxic elements, psychological and emotional factors, and genetics. This holistic evaluation, inspired by the Living Matrix Functional Medicine Assessment, helps identify root causes of chronic disorders and enables truly personalized treatment (Dr. Alex Jimenez, 2025). His dual-scope practice allows him to integrate multiple therapeutic modalities. For RA patients, this might include chiropractic adjustments to improve joint mobility and relieve pain, functional medicine interventions to address gut health and nutritional status, acupuncture or electro-acupuncture to modulate pain and inflammation, and personalized wellness programs incorporating nutrition, exercise, and stress management strategies (Dr. Alex Jimenez, 2025). Dr. Jimenez emphasizes that his approach is collaborative and patient-centered. He works closely with rheumatologists, orthopedic specialists, and other medical providers to ensure coordinated care. If he believes another specialist would better serve a patient’s needs, he provides appropriate referrals, ensuring patients receive the highest standard of care (Dr. Alex Jimenez, 2025). His practice philosophy aligns with evidence-based treatment protocols and focuses on restoring health naturally whenever possible. For RA patients, this means using non-invasive protocols as a priority while recognizing that pharmaceutical interventions may be necessary. The goal is to help patients achieve optimal health through a combination of approaches tailored to their individual needs and circumstances (Dr. Alex Jimenez, 2025).
Functional Wellness Strategies to Combat Rheumatoid Arthritis Symptoms
While chiropractic care addresses mechanical and neurological aspects of RA, functional wellness strategies target the underlying biochemical and lifestyle factors that influence disease activity. A truly comprehensive approach combines both elements.
Anti-Inflammatory Nutrition: The Foundation of Functional Wellness
Diet plays a powerful role in modulating inflammation, and emerging evidence suggests that nutritional interventions can significantly improve outcomes for people with RA. The functional medicine approach to nutrition for RA is highly individualized, recognizing that different people may have different trigger foods and nutritional needs. The Mediterranean diet has received particular attention in RA research. This dietary pattern emphasizes fruits, vegetables, whole grains, fish, olive oil, nuts, seeds, beans, and peas while limiting processed foods and red meat. Research shows that the Mediterranean diet can lower inflammation and improve RA symptoms. In one study, women with RA who followed a Mediterranean-type diet for 6 weeks experienced less joint pain and morning stiffness, as well as better overall health, compared to a control group (The Best and Worst Foods for Rheumatoid Arthritis, 2024). Omega-3 fatty acids, which are abundant in the Mediterranean diet, deserve special attention. These healthy fats, found in fatty fish like salmon, mackerel, and sardines, as well as in flaxseeds and walnuts, have well-documented anti-inflammatory properties. They work by modifying the synthesis of pro-inflammatory eicosanoids, cytokines, and reactive oxygen species. Clinical studies have shown that omega-3 supplementation can decrease morning stiffness, reduce the number of tender joints, and lower the need for NSAIDs in RA patients (Omega-3 Fatty Acids and Vitamin D Improves Inflammatory Biomarkers, 2025). A meta-analysis found that consuming 2.7 grams of EPA/DHA daily for 3 months significantly decreased inflammatory markers, such as interleukin-6 and C-reactive protein, as well as overall disease activity. Higher dietary intake of omega-3 fatty acids during the year preceding DMARD initiation has been associated with better treatment results in patients with early RA (Are dietary vitamin D, omega-3 fatty acids, and folate associated with treatment response?, 2017). The autoimmune protocol (AIP) diet is a more restrictive anti-inflammatory approach that may be helpful for some RA patients. This diet eliminates potential inflammatory triggers, including grains, dairy, eggs, legumes, nightshade vegetables, coffee, alcohol, nuts, seeds, refined sugars, and processed oils. Instead, it focuses on freshly prepared, nutrient-dense foods, fermented foods, and bone broth to support gut health. After a period of strict elimination, foods are gradually reintroduced to identify individual dietary triggers (Integrative Approaches to the Testing and Treatment of Rheumatoid Arthritis, 2025).
Specific foods and nutrients have been identified as particularly beneficial for RA:
Colorful fruits and vegetables are packed with antioxidants and phytonutrients that help combat oxidative stress and inflammation. Berries, leafy greens like spinach and kale, and colorful vegetables like broccoli, beets, and carrots are particularly beneficial. These foods provide vitamins, minerals, and plant compounds that support immune function and reduce inflammation (Embracing an Anti-inflammatory Diet for Rheumatoid Arthritis, 2009).
Beans and legumes are rich in fiber, which can help lower C-reactive protein levels and support a healthy gut microbiome. They also provide plant-based protein to maintain muscle mass around joints. Red beans, kidney beans, pinto beans, lentils, and chickpeas are excellent choices (The Best and Worst Foods for Rheumatoid Arthritis, 2024).
Herbs and spices offer concentrated anti-inflammatory compounds. Turmeric contains curcumin, which has potent anti-inflammatory properties when combined with black pepper (which contains piperine to enhance absorption). Ginger, which is related to turmeric, may have similar effects. Other beneficial spices include clove, coriander, garlic, and capsaicin from chili peppers (Rheumatoid Arthritis Diet, 2013).
Healthy fats from sources like olive oil and avocados provide monounsaturated fats that can help reduce inflammation. Extra virgin olive oil also contains oleocanthal, a compound with anti-inflammatory properties similar to ibuprofen (Embracing an Anti-inflammatory Diet for Rheumatoid Arthritis, 2009).
On the flip side, certain foods may worsen inflammation and should be limited or avoided:
Processed foods and refined sugars can spike blood sugar levels and trigger inflammatory responses. They also provide empty calories without the nutrients needed to support immune function (Integrative Approaches to the Testing and Treatment of Rheumatoid Arthritis, 2025).
Refined vegetable oils high in omega-6 linoleic acid, such as corn, safflower, sunflower, and cottonseed oils, can promote inflammation when consumed in excess relative to omega-3 fats (Integrative Approaches to the Testing and Treatment of Rheumatoid Arthritis, 2025).
Conventionally-raised red meat may contribute to inflammation, particularly when consumed in large amounts. Grass-fed options are preferable if red meat is consumed (Integrative Approaches to the Testing and Treatment of Rheumatoid Arthritis, 2025).
Potential food sensitivities vary by individual but commonly include gluten, dairy, eggs, and nightshade vegetables (tomatoes, peppers, eggplant, white potatoes) for some people with RA. An elimination and reintroduction protocol can help identify personal trigger foods.
A functional medicine study examined the impact of a 12-week nutritional program on RA patients. The program focused on improving nutrition and digestive function, removing inflammatory triggers, and supporting gut health through diet modifications and targeted supplementation. Patients in the functional medicine group showed statistically significant improvements in pain, physical, and mental health scores compared with those receiving standard care alone (The impact of functional medicine on patient-reported outcomes, 2020).
Supporting Gut Health and the Microbiome
Given the strong evidence linking gut dysbiosis to RA, supporting gut health is a crucial component of functional wellness strategies. Several approaches can help restore a more balanced microbiome:
Probiotic supplementation may help increase beneficial bacteria, such as Lactobacillus and Bifidobacterium. Some research suggests that specific probiotic strains can modulate immune responses and reduce systemic inflammation. However, the optimal strains, doses, and treatment duration are still being investigated (Rheumatoid arthritis and the intestinal microbiome, 2024).
Prebiotic fiber feeds beneficial gut bacteria and supports their growth. High-fiber foods like vegetables, fruits, whole grains, and legumes provide the substrate that good bacteria need to produce beneficial metabolites, such as butyrate. Supplemental prebiotic fibers such as inulin, fructooligosaccharides, or partially hydrolyzed guar gum may also be helpful (Integrative Approaches to the Testing and Treatment of Rheumatoid Arthritis, 2025).
Fermented foods like yogurt, kefir, sauerkraut, kimchi, and kombucha contain live beneficial bacteria and may help diversify the gut microbiome. These traditional foods have been consumed for centuries in various cultures and are increasingly recognized for their health benefits (Integrative Approaches to the Testing and Treatment of Rheumatoid Arthritis, 2025).
Bone broth is rich in gelatin, collagen, and amino acids, such as glutamine, that support intestinal barrier function. While more research is needed, many functional medicine practitioners recommend bone broth as part of a gut-healing protocol (Integrative Approaches to the Testing and Treatment of Rheumatoid Arthritis, 2025).
Reducing factors that harm the microbiome is equally important. This includes minimizing unnecessary antibiotic use, avoiding artificial sweeteners and emulsifiers that may negatively affect gut bacteria, managing stress, and limiting alcohol consumption.
The Critical Role of Vitamin D and Other Nutrients
Vitamin D deficiency is highly prevalent in RA patients and has been linked to chronic pain and lower quality of life scores. Multiple studies have found associations between vitamin D status and RA disease activity, suggesting that optimizing vitamin D levels may be an important therapeutic strategy (Can Vitamin D Help Relieve Your Rheumatoid Arthritis?, 2018). Research has shown that vitamin D supplementation can improve disease activity scores and reduce inflammatory markers in RA patients. One randomized controlled trial found that 60,000 IU per week of vitamin D3 for eight weeks significantly improved Disease Activity Score-28 (DAS-28) scores and reduced levels of IL-17 and TNF-α compared to placebo. Higher dietary vitamin D intake during the year before starting DMARD treatment has been associated with better treatment outcomes (Omega-3 Fatty Acids and Vitamin D Improves Inflammatory Biomarkers, 2025). Vitamin D helps regulate immune function through multiple mechanisms. T cells and B cells have vitamin D receptors, indicating direct immunomodulatory effects. Vitamin D appears to help balance Th1 and Th17 immune responses, which are often overactive in RA, while supporting regulatory T cells that help maintain immune tolerance (Omega-3 Fatty Acids and Vitamin D Improves Inflammatory Biomarkers, 2025). For most adults, 1,000-2,000 IU daily of vitamin D3 is recommended for maintenance, though higher doses may be needed initially to correct deficiency. Blood testing of 25(OH)D levels can help guide appropriate dosing. Functional medicine practitioners typically aim for levels between 40 and 60 ng/mL, though optimal targets may vary by individual (Omega-3 Fatty Acids and Vitamin D Improves Inflammatory Biomarkers, 2025).
Other important nutrients for RA management include:
Magnesium plays a role in numerous enzymatic reactions and may help with sleep quality and muscle relaxation. Many people with RA are deficient in magnesium, and supplementation may improve sleep quality (Improving Sleep Quality with Autoimmune Disease, 2025).
Selenium is an antioxidant mineral that supports immune function and may help reduce oxidative stress in RA.
Zinc is crucial for immune system function and wound healing. However, supplementation should be monitored as excessive zinc can interfere with copper absorption.
B vitamins, particularly folate and B12, are important for patients taking methotrexate, as this medication can interfere with folate metabolism. Adequate folate intake may help reduce methotrexate side effects without compromising its effectiveness (Are dietary vitamin D, omega-3 fatty acids, and folate associated with treatment response?, 2017).
Exercise and Physical Activity: Moving Despite the Pain
Regular physical activity is one of the most beneficial interventions for people with RA, yet pain and fatigue often create barriers to exercise. Research consistently shows that appropriate exercise helps relieve RA symptoms and improve day-to-day functioning without exacerbating disease activity (Best Exercises for Rheumatoid Arthritis, 2023).
The benefits of exercise for RA patients are multifaceted. Physical activity helps reduce pain and stiffness, improve joint mobility and function, maintain or increase muscle strength, enhance cardiovascular fitness, support weight management, reduce fatigue, improve sleep quality, and boost mood and overall well-being (Role of physical activity in the management, 2017).
A comprehensive exercise program for RA should incorporate several components:
Range-of-motion and flexibility exercises help maintain or improve joint mobility and reduce stiffness. These should be performed daily and include gentle stretching of all major joints. During acute flares, when joints are actively inflamed, range-of-motion exercises should be gentle and pain-free. As inflammation subsides, more active stretching can be incorporated (Physiotherapy in Rheumatoid Arthritis, 2004).
Strengthening exercises help maintain muscle mass and joint stability. Isometric exercises, where muscles contract without moving the joint, are particularly valuable during periods of active inflammation. These exercises can be performed at relatively low intensity (40% of maximum voluntary contraction) and held for 6 seconds, repeated 5-10 times daily. As disease activity improves, progressive resistance training with light weights or resistance bands can be added (Physiotherapy in Rheumatoid Arthritis, 2004).
Aerobic conditioning improves cardiovascular health, increases muscle endurance, and helps manage fatigue. Low-impact activities like swimming, walking, cycling, water aerobics, and tai chi are excellent options. Moderate-intensity aerobic exercise for 30 minutes, five times per week, or intensive exercise for 20 minutes, three times per week, can provide significant benefits (Rheumatoid Arthritis, 2024).
Balance and coordination exercises help prevent falls and improve functional capacity. Activities like tai chi, gentle yoga, and standing on balance boards stimulate the sensorimotor system and enhance joint stability (Rheumatoid Arthritis, 2024).
Important principles for exercising with RA include:
Start slowly and progress gradually
Listen to your body and respect pain signals
Avoid exercise during acute flares of highly inflamed joints
Include adequate rest periods
Stop if pain persists for more than two hours after exercise or if you experience increased swelling, loss of strength, or excessive fatigue
Work with a physical therapist to develop an individualized program
Choose activities you enjoy to enhance long-term adherence
Recent research has shown an interesting bidirectional relationship between physical activity and disease activity. Changes in RA disease activity inversely correlate with variations in physical activity—when disease activity increases, physical activity tends to decrease, and vice versa. This suggests that monitoring physical activity levels may provide valuable information about disease status (Role of physical activity in the management, 2017).
Sleep Optimization: The Underestimated Healing Tool
Up to 70% of people with RA experience sleep problems, and poor sleep quality can significantly worsen disease symptoms. Sleep disturbances and RA create a vicious cycle: pain and inflammation disrupt sleep, and poor sleep increases pain sensitivity and inflammatory markers, which further exacerbate RA symptoms (Understanding the Relationship Between Rheumatoid Arthritis and Sleep, 2023). The relationship between sleep and inflammation is complex and bidirectional. During sleep, the body engages in critical repair and restoration processes. The immune system uses this time to produce and distribute certain immune cells and anti-inflammatory molecules. Sleep deprivation disrupts these processes, leading to increased production of pro-inflammatory cytokines and decreased production of anti-inflammatory mediators (The Importance of Sleep Hygiene, 2024). Research shows that acute sleep deprivation correlates with increased pain and arthritis symptoms the following day. Conversely, improved sleep quality is associated with reduced pain sensitivity, better pain management, lower inflammatory markers, improved immune regulation, enhanced mood and cognitive function, and increased energy levels (10 Tips to Improve Sleep with Rheumatoid Arthritis, 2023). Strategies to improve sleep quality in RA include:
Pain management is fundamental. Working with your healthcare team to optimize pain control helps you sleep more restfully. Taking medications at appropriate times, using heat or cold therapy before bed, ensuring comfortable sleeping positions with supportive pillows, and practicing gentle stretching before bed may all help (Understanding the Relationship Between Rheumatoid Arthritis and Sleep, 2023).
Establishing a consistent sleep routine helps regulate your body’s internal clock. Go to bed and wake up at the same time each day, even on weekends. Create a relaxing pre-bedtime routine that might include reading, meditation, gentle stretching, or taking a warm bath (The Importance of Sleep Hygiene, 2024).
Optimizing your sleep environment can make a significant difference. Keep your bedroom cool (around 65-68°F), dark, and quiet. Use blackout curtains or an eye mask if needed. Consider a white noise machine if you’re sensitive to sounds. Invest in a supportive mattress and pillows that accommodate your specific needs (Improving Sleep Quality with Autoimmune Disease, 2025).
Practicing good sleep hygiene means avoiding caffeine and alcohol in the evening, limiting screen time before bed (blue light from devices can suppress melatonin production), avoiding large meals close to bedtime, getting regular exercise but not too close to bedtime, and keeping the bedroom for sleep and intimacy only (The Importance of Sleep Hygiene, 2024).
Managing stress and mental health is crucial, as anxiety and depression commonly accompany RA and can significantly disrupt sleep. Techniques like deep breathing, progressive muscle relaxation, mindfulness meditation, and cognitive-behavioral therapy for insomnia (CBT-I) can be very effective. Seeking support from a therapist or support group may also help (Understanding the Relationship Between Rheumatoid Arthritis and Sleep, 2023).
Sleep aids and supplements may be appropriate for some individuals. Melatonin can help regulate sleep-wake cycles and may have additional anti-inflammatory properties. Magnesium supports muscle relaxation and sleep quality. Herbal teas like chamomile may promote relaxation. However, always consult with your healthcare provider before starting any new supplement, as some may interact with RA medications (Improving Sleep Quality with Autoimmune Disease, 2025).
Stress Management and Mind-Body Techniques
Chronic stress is both a contributing factor to RA development and a consequence of living with the disease. Stress triggers the release of cortisol and other hormones that can promote inflammation and suppress immune function. Additionally, stress can worsen pain perception, disrupt sleep, and negatively impact overall quality of life (5 Ways Chiropractic Care Can Support Autoimmune Disease Management, 2025).
Mind-body techniques offer powerful tools for managing stress and improving well-being:
Mindfulness meditation involves paying attention to the present moment without judgment. Research has shown that mindfulness practices can reduce pain, decrease stress and anxiety, improve sleep quality, enhance emotional regulation, and reduce inflammatory markers. Even brief daily sessions of 10-20 minutes can provide benefits (incorporating wellness practices, 2021).
Deep breathing exercises activate the parasympathetic nervous system, promoting relaxation and countering the stress response. Techniques like diaphragmatic breathing, box breathing (inhaling for 4 counts, holding for 4, exhaling for 4, holding for 4), or extended exhalation (inhaling for 4 counts, exhaling for 6-8 counts) can be practiced anywhere and provide immediate calming effects.
Progressive muscle relaxation involves systematically tensing and then relaxing different muscle groups throughout the body. This technique helps increase body awareness, reduce muscle tension, and promote overall relaxation.
Tai chi is a gentle movement practice combining flowing movements, deep breathing, and meditation. Multiple studies have found that tai chi can improve mood, quality of life, pain, and physical function in people with RA. When taught by a qualified instructor, tai chi is safe for most people with RA, though movements should be modified to avoid positions that cause pain (Rheumatoid arthritis – Diagnosis and treatment, 2025).
Yoga offers another mind-body approach that may benefit people with RA. Gentle or restorative yoga practices can improve flexibility, strength, balance, and stress management. As with tai chi, it’s important to work with an instructor experienced in working with people who have chronic pain or arthritis.
Biofeedback and neurofeedback are techniques that help people learn to control certain physiological processes through real-time feedback. These approaches can be helpful for pain management and stress reduction.
Cognitive-behavioral therapy (CBT) addresses the thoughts and behaviors that contribute to pain and distress. CBT has been shown to help people with chronic pain develop better coping strategies, reduce pain-related disability, and improve quality of life.
Additional Non-Surgical Treatments and Practical Strategies for Symptom Relief
Beyond the foundational strategies of nutrition, exercise, sleep, and stress management, several additional approaches can help reduce RA symptoms and improve daily functioning.
Heat and Cold Therapy
Applying heat or cold to affected joints can provide significant relief:
Heat therapy helps relax muscles, increase blood flow, and reduce stiffness. Warm baths, heating pads, warm paraffin wax treatments, and moist heat packs can all be beneficial. Heat is generally most helpful for chronic stiffness and before activity (Physiotherapy in Rheumatoid Arthritis, 2004).
Cold therapy helps reduce inflammation, numb pain, and decrease swelling. Ice packs, cold compresses, or cool water immersion can be used for 15-20 minutes at a time. Cold is often most helpful during acute flares or after activity (Physiotherapy in Rheumatoid Arthritis, 2004).
Some people find contrast therapy—alternating between heat and cold—particularly helpful for reducing stiffness and improving circulation.
Assistive Devices and Joint Protection
Using appropriate assistive devices and practicing joint protection techniques can significantly reduce strain on affected joints and improve function:
Ergonomic tools like jar openers, built-up handles on utensils, reachers, and button hooks make daily tasks easier without stressing joints.
Braces and splints can provide support, reduce pain, and prevent deformity. Wrist splints, finger splints, knee braces, and ankle-foot orthoses may all be beneficial depending on which joints are affected.
Proper footwear is crucial for people with foot involvement. Shoes should have good arch support, cushioning, and a wide toe box. Custom orthotics may be recommended by a podiatrist.
Joint protection principles include using larger, stronger joints when possible, avoiding positions that push joints toward deformity, taking frequent breaks during activities, planning ahead to conserve energy, and using good body mechanics and posture.
Occupational and Physical Therapy
Working with occupational and physical therapists can provide tremendous benefits:
Occupational therapists help with activities of daily living, recommend assistive devices, teach joint protection techniques, and provide hand therapy, including exercises and splinting.
Physical therapists develop individualized exercise programs, provide manual therapy, teach proper body mechanics, and help with pain management strategies.
Both types of therapy have strong evidence supporting their use in RA management and should be considered part of comprehensive care (Rehabilitation Management for Rheumatoid Arthritis Patients, 2012).
Complementary Therapies
Several complementary therapies have shown promise for RA symptom management:
Acupuncture involves inserting thin needles at specific points on the body. Some studies suggest it can help reduce pain and improve joint function in RA, though more research is needed (Exploring Alternative Treatments for Rheumatoid Arthritis, 2024).
Massage therapy can help alleviate pain, reduce muscle tension, improve circulation, and promote relaxation. Working with a licensed massage therapist experienced in treating people with RA is important (Exploring Alternative Treatments for Rheumatoid Arthritis, 2024).
Hydrotherapy or aquatic therapy takes advantage of the buoyancy and resistance of water. Warm water exercise can improve strength and range of motion while minimizing joint stress (Physiotherapy in Rheumatoid Arthritis, 2004).
Lifestyle Modifications
Small changes to daily habits can add up to significant improvements:
Energy conservation involves pacing activities, planning ahead, prioritizing tasks, and taking regular rest breaks to manage fatigue.
Stress reduction techniques should be incorporated into daily life, not just practiced during dedicated sessions. This might include brief breathing exercises throughout the day, listening to calming music, spending time in nature, or engaging in hobbies.
Social connection is important for both emotional and physical health. Maintaining relationships, participating in support groups, and staying engaged with community can all support better outcomes.
Avoiding smoking is crucial, as smoking not only increases RA risk but also reduces the effectiveness of treatments and increases disease severity. If you smoke, quitting is one of the most important steps you can take.
Limiting alcohol is also advisable, as alcohol can interfere with RA medications and may exacerbate inflammation and gut dysbiosis.
Integrating Chiropractic Care with Functional Wellness: A Holistic Framework
The most effective approach to managing RA combines multiple strategies tailored to each individual’s unique needs, circumstances, and preferences. Dr. Jimenez’s integrated model exemplifies how chiropractic care and functional wellness can work together synergistically. In this model, chiropractic adjustments and manual therapy address the mechanical and neurological aspects of the condition—improving joint mobility, reducing mechanical stress, supporting nervous system function, and providing pain relief. Meanwhile, functional medicine interventions target the underlying biochemical and lifestyle factors—optimizing nutrition and gut health, correcting nutrient deficiencies, supporting detoxification pathways, and addressing environmental triggers (Dr. Alex Jimenez, 2025). This comprehensive approach recognizes that RA is a multifactorial disease requiring multifactorial solutions. No single intervention is likely to be sufficient on its own, but combining evidence-based therapies can yield meaningful improvements in symptoms, function, and quality of life. The functional medicine assessment process begins with an extensive evaluation. Practitioners take a detailed medical history from birth, explore dietary and lifestyle patterns, assess environmental exposures at home, work, and leisure, evaluate digestive health and gut symptoms, review stress levels and mental health, examine hormonal function, and analyze genetic predispositions when relevant (Rheumatoid Arthritis Treatment – Melbourne Functional Medicine, 2025). With this comprehensive picture, a personalized treatment plan is developed that might include dietary modifications to remove triggers and emphasize anti-inflammatory foods, targeted nutritional supplements to address deficiencies and support immune function, gut health interventions including probiotics, prebiotics, and gut-healing nutrients, stress management and mind-body techniques, sleep optimization strategies, appropriate exercise programming, and environmental modifications to reduce toxic exposures (Rheumatoid Arthritis Treatment – Melbourne Functional Medicine, 2025). Regular monitoring and adjustment of the treatment plan ensure that it continues to meet the patient’s evolving needs. This might involve periodic laboratory testing to assess inflammatory markers, nutrient status, and other relevant biomarkers, reassessment of symptoms and functional capacity, and modification of interventions based on response (Rheumatoid Arthritis Treatment – Melbourne Functional Medicine, 2025). Throughout this process, communication and coordination with the patient’s rheumatologist and other healthcare providers are essential. The goal is not to replace conventional medical treatment but to complement it, potentially enhancing its effectiveness while addressing aspects of health that may not be the primary focus of standard rheumatology care.
Conclusion: Empowering Your Journey with Rheumatoid Arthritis
Living with rheumatoid arthritis is hard all the time, but knowing more about the disease and having access to a wide range of treatment options can make a big difference. Chiropractic care and functional wellness strategies together can help you better manage your symptoms, improve your function, and enhance your quality of life. The evidence examined in this article indicates that rheumatoid arthritis (RA) is not merely a joint disorder but a multifaceted systemic condition affected by genetic predispositions, environmental exposures, gastrointestinal health, nutritional status, stress levels, and lifestyle decisions. This comprehension facilitates a multitude of intervention opportunities beyond traditional pharmaceutical methods. Chiropractic care can safely improve joint mobility, reduce pain, support nervous system function, and help manage the mechanical aspects of RA when provided by practitioners who have experience with autoimmune conditions. Clinical studies have shown that manual therapy techniques that are specifically designed for people with RA can be helpful and should be a part of comprehensive care. Functional wellness strategies, such as anti-inflammatory nutrition, gut health support, targeted supplementation, appropriate exercise, sleep optimization, and stress management, address the fundamental factors that influence disease activity and symptoms. The new studies on the gut-joint axis, the roles of vitamin D and omega-3 fatty acids, and the microbiome in autoimmune disease provide these treatments with a scientific basis. Dr. Alexander Jimenez’s integrated approach shows how these different parts can work together to make a complete treatment plan. He is a chiropractor and a nurse practitioner, and he is also certified in functional medicine. This means he can provide care that covers both the structural and biochemical aspects of chronic inflammatory conditions. The message for patients is one of hope and strength. You have more control over your health than you might think, even though RA is a serious condition that needs ongoing medical care. The decisions you make about what you eat, how you move, how you handle stress, and how you support your body’s healing can have a big impact on how your disease progresses and how good your life is. To manage RA well, you need a full range of support from a healthcare team that includes your rheumatologist, a chiropractor who understands inflammatory conditions, and functional medicine practitioners. This team-based approach, along with your active participation in self-care strategies, gives you the best chance of getting the best results. It’s important to remember that dealing with RA is a journey, not a destination. It may take time to make progress, and there will probably be setbacks along the way. But many people with RA can lessen their symptoms, get better at doing things, and live full, meaningful lives with the right support, patience, and determination.
Gibofsky, A. (2014). Epidemiology, pathophysiology, and diagnosis of rheumatoid arthritis: A synopsis. American Journal of Managed Care, 20(7 Suppl), S128-S135.
Gut-joint axis: Gut dysbiosis can contribute to the onset of rheumatoid arthritis via multiple pathways. (2023). Frontiers in Cellular and Infection Microbiology, 13, 1092118. https://doi.org/10.3389/fcimb.2023.1092118
Jang, S., Kwon, E.-J., & Lee, J. J. (2022). Rheumatoid arthritis: Pathogenic roles of diverse immune cells. International Journal of Molecular Sciences, 23(2), 905. https://doi.org/10.3390/ijms23020905
Manual Therapy (Postisometric Relaxation and Joint Mobilization) in Knee Pain and Function Experienced by Patients with Rheumatoid Arthritis: A Randomized Clinical Pilot Study. (2020). PMC – National Center for Biotechnology Information. https://pmc.ncbi.nlm.nih.gov/articles/PMC7453239/
The impact of functional medicine on patient-reported outcomes in rheumatoid arthritis. (2020). PMC – National Center for Biotechnology Information. https://pmc.ncbi.nlm.nih.gov/articles/PMC7544031/
Wasserman, A. M. (2011). Diagnosis and management of rheumatoid arthritis. American Family Physician, 84(11), 1245-1252.
Important Disclaimer
This article is intended for educational and informational purposes only and should not be construed as medical advice. The information presented here is based on current research and clinical perspectives, but rheumatoid arthritis is a serious medical condition that requires professional diagnosis and treatment.
Please note the following:
Do not use this information to diagnose or treat any health condition. If you suspect you have rheumatoid arthritis or are experiencing joint pain, swelling, or other concerning symptoms, consult with a qualified healthcare provider, preferably a rheumatologist, for proper evaluation and diagnosis.
Do not stop or modify prescribed medications without consulting your physician. Disease-modifying antirheumatic drugs (DMARDs) and other medications prescribed for RA are essential for controlling disease activity and preventing joint damage. The approaches discussed in this article are intended to complement, not replace, conventional medical treatment.
Always inform your healthcare team about all treatments you are using, including chiropractic care, supplements, dietary changes, and other complementary therapies. This ensures coordinated care and helps prevent potential interactions or complications.
Individual results may vary. The research and clinical experiences described in this article represent general findings that may not apply to every individual. Your response to any treatment approach will depend on numerous factors, including disease severity, presence of other medical conditions, medications, and individual characteristics.
Chiropractic care and manual therapy should be performed only by licensed, trained professionals with experience treating patients with inflammatory arthritis. Not all techniques are appropriate for all patients, and adjustments must be carefully tailored to each individual’s condition.
Some supplements and dietary approaches may interact with RA medications or may not be appropriate for individuals with certain medical conditions. Always consult with your healthcare provider before starting any new supplement regimen.
This article was prepared with care based on available research and clinical expertise, but medical knowledge continues to evolve. The information provided should be considered in the context of your individual situation and in consultation with qualified healthcare professionals who can evaluate your specific needs and circumstances.
If you are experiencing a medical emergency, call 911 or seek immediate medical attention. Do not rely on information from this or any online article in emergency situations.
Written with clinical insights from Dr. Alexander Jimenez, DC, APRN, FNP-BC, CFMP, IFMCP, who specializes in integrative approaches to chronic pain and inflammatory conditions through chiropractic care and functional medicine at El Paso’s Premier Wellness and Injury Care Clinic.
Eat to Help a Herniated Disc: Protein, Omega-3s, Vitamins, Minerals, and Hydration for Faster, Healthier Spine Recovery
Overview
What you eat can help your spine heal. Foods rich in protein, omega-3 fatty acids, vitamins, and minerals support tissue repair, calm inflammation, and keep your spinal discs healthy and hydrated. When you pair smart nutrition with integrative care—like chiropractic adjustments and non-invasive decompression—you can lower disc pressure, improve nerve function, and speed recovery. This guide explains how to build a spine-friendly plate and water routine that works in real life. (National Spine Health Foundation, 2024; Texas Back Institute, n.d.; Jimenez, 2022–2025). El Paso, TX Doctor Of Chiropractic+3National Spine Health Foundation+3Texas Back Institute+3
Why nutrition matters for herniated discs
A herniated disc happens when the soft center of a disc pushes through its outer layer, which can irritate nearby nerves and cause pain, tingling, or weakness. Your body tries to calm the area and rebuild tissue—but it needs raw materials (amino acids, vitamins, and minerals) and fewer inflammatory triggers to do so effectively. A diet centered on lean protein, omega-3-rich foods, colorful produce, nuts, seeds, and whole grains provides these nutrients while helping control inflammation. (Texas Back Institute, n.d.; Healthline, 2021; National Spine Health Foundation, 2024). Texas Back Institute+2Healthline+2
Hydration: the first “nutrient” for discs
Spinal discs are mostly water. They act as shock-absorbing cushions between vertebrae and rely on hydration to stay plump and flexible. When you’re dehydrated, discs lose height and elasticity, which can increase stress on the outer layers and irritate nerves. Drinking water throughout the day helps transport nutrients to discs and supports synovial fluid, which promotes smooth joint motion. Aim for steady intake, not just big gulps once or twice a day. (National Spine Health Foundation, 2024; Jimenez, 2018; ANSSI Wellness, 2025). National Spine Health Foundation+2El Paso, TX Doctor Of Chiropractic+2
Hydration how-to (simple steps):
Keep water visible—on your desk, nightstand, and in the car.
Add water-rich foods like cucumbers, citrus, and melon to meals.
Your spine’s muscles, ligaments, and the collagen network inside discs all rely on amino acids. Getting enough protein helps you rebuild tissue and maintain strength that supports the spine. Good choices include fish, poultry, eggs, Greek yogurt, beans, and lentils. If you eat plant-based foods, mix legumes, soy, and grains to cover essential amino acids. (Texas Back Institute, n.d.; Frisco Spinal Rehab, 2025). Texas Back Institute+1
Collagen support: Collagen and glycine can help rebuild connective tissue. You can get these from bone broth, collagen peptides, or cuts of meat that include cartilage and skin. Plant sources (like soy and beans) also provide amino acids, though you may need a bit more volume to match the totals. (DiscSeel/Dr. Pauza, n.d.; Frisco Spinal Rehab, 2025). Discseel+2drkevinpauza.com+2
Omega-3 fatty acids: dial down inflammation
Omega-3s from fatty fish (salmon, sardines, herring, mackerel, and anchovies), walnuts, chia, and flax help calm the inflammatory pathways that often flare with disc injuries. Many people notice better joint comfort when they replace some omega-6-heavy processed foods with omega-3-rich whole foods. (Healthline, 2019/2021; National Spine Health Foundation, 2024). Healthline+2Healthline+2
If you don’t eat fish, nuts and seeds are solid choices. Chia, flax, and walnuts provide ALA (a plant omega-3), plus fiber and magnesium—both helpful for nerve and muscle function. (417 Spine, 2024). 417spine.com
Vitamins & minerals that support discs, nerves, and bones
Vitamin C
Vitamin C helps your body make collagen—the framework inside discs, ligaments, and other connective tissues. Citrus, berries, bell peppers, and leafy greens are easy ways to get it daily. (Spine Orthopedic Center, 2024). Spine & Orthopedic Center
Vitamin D + Calcium + Magnesium
These nutrients work together. Vitamin D helps you absorb calcium; magnesium helps activate vitamin D and supports bone and muscle function. You’ll find calcium in dairy and fortified plant milks, leafy greens, beans, nuts, and small bony fish (like sardines). Magnesium shows up in spinach, pumpkin seeds, almonds, beans, and whole grains. (National Spine Health Foundation, 2024; National Spine Health Foundation, 2017). National Spine Health Foundation+1
B-vitamins and antioxidants
Colorful fruits and vegetables provide antioxidants that help fight oxidative stress, which can worsen pain and tissue damage. Look for dark leafy greens and bright berries—simple swaps with big payoff. (Illinois Back Institute, 2024; Spine Wellness America, 2024). illinoisbackpain.com+1
What a spine-supportive plate looks like
Build most meals with:
A quality protein (¼ plate): grilled salmon or trout; baked chicken; eggs; or plant options like tofu, tempeh, beans, or lentils. (Texas Back Institute, n.d.; Healthline, 2019). Texas Back Institute+1
Colorful produce (½ plate): leafy greens, cruciferous vegetables, tomatoes, and berries for vitamin C, vitamin K, antioxidants, and fiber. (Bonati Spine Institute, 2021; Illinois Back Institute, 2024). Bonati Spine Institute+1
Whole grains or starchy veggies (¼ plate): quinoa, brown rice, oats, winter squash, or sweet potatoes to fuel healing and provide magnesium and potassium. (National Spine Health Foundation, 2024). National Spine Health Foundation
Snack ideas: Greek yogurt with berries; a small handful of mixed nuts and seeds; hummus with carrots and cucumbers; chia pudding; or a bone-broth mug for extra collagen. (DiscSeel/Dr. Pauza, n.d.; 417 Spine, 2024). Discseel+1
Simple 1-day starter menu (easy high-school level)
Breakfast: Greek yogurt parfait with blueberries, sliced almonds, and a sprinkle of chia; water or green tea.
Lunch: Salmon salad over spinach and kale with cherry tomatoes, quinoa, olive oil vinaigrette, and sliced orange.
Snack: Bone broth or collagen smoothie (banana + spinach + collagen peptides + water).
Dinner: Turkey chili with beans and bell peppers; side of roasted broccoli; whole-grain tortilla; water.
Hydration goal: Fill a 24-oz bottle and finish it twice by dinner, then have another glass in the evening. (Healthline, 2019; National Spine Health Foundation, 2024; DiscSeel/Dr. Pauza, n.d.). Healthline+2National Spine Health Foundation+2
Foods to emphasize for herniated disc recovery
Fatty fish (salmon, sardines, mackerel, herring, and anchovies): protein + omega-3s to reduce inflammation. (Healthline, 2019). Healthline
Berries (blueberries, strawberries, blackberries): vitamin C and polyphenols to support collagen and calm oxidative stress. (Florida Spine Associates, 2021). Florida Spine Associates
Leafy greens (spinach, kale, and collards): magnesium, vitamin K, and antioxidants for bone and connective tissue health. (Spine Orthopedic Center, 2024). Spine & Orthopedic Center
Nuts and seeds (walnuts, almonds, chia, flax): healthy fats, magnesium, and fiber—great for inflammation control and nervous system support. (417 Spine, 2024). 417spine.com
Lean meats, eggs, yogurt, beans, and lentils: protein for repair; pair with produce for vitamins that drive collagen synthesis. (Texas Back Institute, n.d.; Frisco Spinal Rehab, 2025). Texas Back Institute+1
Bone-broth or collagen (optional): extra glycine/proline to support connective tissue repair. (DiscSeel/Dr. Pauza, n.d.). Discseel
Foods and habits to limit
Most people do best limiting refined sugars, ultra-processed foods, and excessive alcohol or caffeine, which can worsen inflammation or interfere with calcium balance and hydration. Choose whole foods most of the time. (National Spine Health Foundation, 2024; Verywell Health, 2024). National Spine Health Foundation+1
How nutrition and chiropractic integrative care work together
Chiropractic adjustments and gentle spinal decompression can reduce disc pressure, improve nerve flow, and help you move with less pain—all without surgery. When you combine these treatments with targeted nutrition and hydration, you may get better, faster results because well-nourished tissues hold adjustments longer and repair more efficiently. (Jimenez, 2022–2025). El Paso, TX Doctor Of Chiropractic+2El Paso, TX Doctor Of Chiropractic+2
Clinical observations (Dr. Alexander Jimenez, DC, APRN, FNP-BC): In practice, Dr. Jimenez emphasizes:
Nutrition with care plans—anti-inflammatory foods, adequate protein, and minerals alongside adjustments and decompression. (Jimenez, 2022–2025). El Paso, TX Doctor Of Chiropractic+1
Dual-scope, integrative approach using lifestyle guidance plus hands-on care, with imaging and diagnostics when needed to guide safe rehab. (Jimenez, LinkedIn profile). LinkedIn
FAQs
Do I need an omega-3 supplement? Food first is best. If you don’t eat fish, ask your clinician about algae-based DHA/EPA or fish oil, and about medication interactions (such as blood thinners). (Verywell Health, 2023). Verywell Health
Can protein help even if I’m not post-surgery? Yes. Protein supports the daily repair of muscles and connective tissues around the spine. Most people with disc pain benefit from steady protein at each meal. (Texas Back Institute, n.d.). Texas Back Institute
Are nuts and seeds okay if I’m watching calories? Yes—use small portions (about a small handful). They deliver fiber, magnesium, and healthy fats that support nerve and muscle function and help control inflammation. (417 Spine, 2024). 417spine.com
How much water should I drink? There’s no one perfect number, but sipping regularly and watching the color of your urine (pale yellow) is a simple guide. Increase intake with heat, exercise, or high-fiber meals. (National Spine Health Foundation, 2024; ANSSI Wellness, 2025). National Spine Health Foundation+1
7-day “spine stack” checklist
Daily: Fill a large bottle 2–3 times; include leafy greens and berries; add one omega-3 food; include a palm-sized protein each meal. (National Spine Health Foundation, 2024; Healthline, 2019). National Spine Health Foundation+1
3× per week: Fatty fish or plant omega-3 + nuts/seeds. (Healthline, 2019; 417 Spine, 2024). Healthline+1
Weekly prep: Make a batch of bone broth or pick up collagen peptides if recommended. (DiscSeel/Dr. Pauza, n.d.). Discseel
Care synergy: Keep chiropractic visits, do your home exercises, and bring questions about diet or supplements to your clinician. (Jimenez, 2022–2025). El Paso, TX Doctor Of Chiropractic+1
Putting it all together
Eating for a herniated disc is not about perfection. It’s about steady hydration and building most meals around protein, omega-3s, minerals, and colorful plants. Pair that with chiropractic integrative care—like adjustments and non-invasive decompression—and you give your spine the best chance to calm inflammation, protect nerves, and rebuild tissues. Start with one habit today: fill your water bottle, plan a salmon-and-greens dinner, or add a handful of walnuts to your yogurt. Small steps add up. (National Spine Health Foundation, 2024; Jimenez, 2022–2025; Healthline, 2019). Healthline+3National Spine Health Foundation+3El Paso, TX Doctor Of Chiropractic+3
References
ANSSI Wellness. (2025, Sept). How dehydration affects your spine and leads to neck pain.anssiwellness.com
ANSSI Wellness. (2025, Aug). Bulging disc recovery diet – best foods for spine healing.anssiwellness.com
Bonati Spine Institute. (2021, May 10). 5 best foods for your spine health.Bonati Spine Institute
DiscSeel / Pauza, K. (n.d.). Herniated disc: Natural treatment.Discseel
Florida Spine Associates. (2021, Dec 10). Foods for spine surgery recovery: What to eat and avoid.Florida Spine Associates
Frisco Spinal Rehab. (2025, Sept 15). The best diet for spinal disc recovery and faster healing.Frisco Spinal Rehab
Frisco Spinal Rehab. (2025, Sept 2). Glycine: The hidden nutrient for spinal disc healing.Frisco Spinal Rehab
ChiroMed’s Integrative Approach to Digestion, Nutrition, and Cleansing in El Paso
Many residents of El Paso frequently experience stomach pain, slow bowel movements, or persistent bloating that disrupt their daily activities. These signs point to gut trouble that affects energy and mood. At ChiroMed – Integrated Medicine Holistic Healthcare in El Paso, Texas, a full-team approach naturally fixes this. Chiropractic care leads the way with gentle spinal adjustments, soft-tissue work, healthy eating plans, and detox support. It all starts with the nervous system—the body’s control center for food breakdown and waste removal. Clear nerve signals mean smoother digestion and fewer aches. Better blood flow brings fresh oxygen to organs. Simple diet and lifestyle tips keep toxins moving out. Together, this process builds strong gut health that lasts.
ChiroMed sees the spine as the main highway to every organ. A small shift in the back can block messages to the stomach or intestines. Adjustments realign bones to free nerves. This helps the brain direct enzymes, muscle waves, and acid levels just right. Patients notice less gas and easier, faster trips to the bathroom. Adding massage and custom food plans speeds the body’s own cleanup system. The result? A lighter belly and more pep in your step.
The gut and liver work as partners. The liver filters junk; the gut sends it there. Nerve blocks slow the team down, causing swelling and fatigue. ChiroMed fixes this link with targeted care. Dr. Alexander Jimenez, the clinic’s lead chiropractor and nurse practitioner, watches these improvements happen every week. He says spine fixes cut swelling and help the gut-liver axis heal (Jimenez, n.d.a). Locals injured in car wrecks or desk jobs find their tummy calm returns when nerves flow free.
Care at ChiroMed goes beyond the table. Guides teach easy meals, water habits, and calm tricks that fit busy El Paso lives. These steps power detox so the body sheds waste through skin, breath, and bowels without harsh cleanses. A personal plan makes change simple and lasting.
Your Nervous System Runs the Show at ChiroMed
Picture wires from your brain to your belly telling it when to churn and when to rest. That is the autonomic nervous system. Stress or incorrect posture can pinch those wires in the spine. The middle back connects straight to the stomach; the lower back links to the colon. A pinch slows everything, leaving food stuck and waste backed up (Hyslop, 2023).
ChiroMed doctors feel for these spots and use light pushes to set them right. No twisting or pain—just quick relief. Nerves open up, and the vagus nerve—the gut’s best friend—takes charge again. This flips the body into rest-and-digest mode. Bloating drops, cramps fade, and food moves on time (Parco of Ontario, n.d.).
Dr. Jimenez shares real stories from the clinic. A teacher with neck pain from grading papers came in bloated every afternoon. Scans showed a thoracic shift pressing the gut nerves. Four adjustments plus breathing homework cleared both issues. Jimenez links it to lower-stress chemicals used to kill beneficial bacteria (Jimenez, n.d.b). Clear signals keep the microbiome happy and the belly quiet.
Spine Adjustments at ChiroMed: Fast Track to Easy Digestion
The primary service offered at ChiroMed is spinal adjustment. Safe, drug-free, and backed by years of results, it realigns the spine so nerves fire correctly. For gut care, the team targets the thoracic and lumbar zones. These nerves go to the stomach, liver, and bowels.
A typical visit starts with posture photos and gentle touch tests. Then comes the adjustment—precise pressure that may make a soft pop. Blood rushes in; nerves wake up. Patients feel looser right away. Studies note up to 50% less heartburn when diaphragm pressure lifts (Well Beings Medicine, n.d.). Constipation eases as colon nerves spark wave-like motion (Abundant Life Chiropractor, n.d.).
El Paso runners love this. A marathon trainer with IBS flares saw stool patterns steady after lumbar work. Dr. Jimenez added core planks to lock in posture gains. No more race-day bathroom panic. Adjustments also address slouching that can squish organs. Standing tall gives the gut room to work.
Circulation Boost: ChiroMed’s Secret to Gut Repair
Healthy blood flow delivers oxygen and nutrients to gut cells. Tight back muscles or spine stress choke it off. Toxins pile up, and healing stalls. ChiroMed opens the pipes.
Adjustments widen vessels near the spine, flooding the belly with fresh blood. This feeds the gut wall and speeds waste to the liver (DC Labs, n.d.). Soft tissue massage melts knots that block flow. Ultrasound waves warm deep layers for an extra rush. Dr. Jimenez tracks progress with simple energy checks—patients report clearer skin and steady pep as detox kicks in (Jimenez, n.d.a).
Daily tips to keep it going: short walks along the Franklin Mountains or yoga at home. These pumps move lymph fluid that sweeps away junk. Less swelling means fewer leaky-gut leaks into the blood.
ChiroMed Nutrition Plans: Eat Smart for El Paso Lifestyles
Food is medicine at ChiroMed. The team builds three-phase plans that fit the tastes of border towns.
Phase 1: Clean – Drop sugar and fried foods to starve bad bugs.
Phase 2: Feed – Add greens, beans, and fermented picks like kimchi from local markets.
Phase 3: Balance – Keep variety with proteins and healthy fats (Touch Chiropractic, n.d.).
Tests spot low good bacteria early. Dr. Jimenez loves salmon tacos with avocado—anti-inflammatory and tasty. Hydration is easy: carry a bottle and aim for clear pee. Stress tools like five-minute breaths calm the vagus nerve between appointments.
Detox the ChiroMed Way: Gentle and Effective
The body detoxes daily—liver, kidneys, skin, lungs. ChiroMed makes it smoother. Adjustments fire up gut push; massage moves lymph; diet binds toxins so they leave, not circle back (Spine and Joint Center, n.d.).
El Paso heat helps—light sweat sessions or home dry saunas flush skin. Rebounding on a mini trampoline bounces waste out. Supplements like milk thistle support the liver only when tests say yes. Dr. Jimenez watches accident patients drop brain fog as toxin loads fall (Jimenez, n.d.c).
Dr. Jimenez Leads ChiroMed with Proven Integrative Care
Dr. Alexander Jimenez, DC, APRN, FNP-BC, IFMCP, founded ChiroMed to blend chiropractic, nursing, and functional medicine under one roof. Thousands of El Paso families trust his care each year.
A construction worker came in after a fall, with back pain plus weeks of constipation. Imaging showed lumbar subluxations. Adjustments, probiotics, and fiber from local nopales fixed them both in six weeks. Lab retests proved diverse gut flora returned (Jimenez, n.d.a). Jimenez calls it the spine-gut axis in action.
His protocols use X-rays, stool studies, and food logs for custom paths. No guesswork—just results. As El Paso’s go-to integrative doctor, he teaches patients to take ownership of their health.
Start Your Gut Journey at ChiroMed Today
ChiroMed – Integrated Medicine Holistic Healthcare offers El Paso a clear road to gut comfort. Begin with a full spine and gut check. Adjustments clear nerve noise; therapies and plans lock in gains. Eat, move, and breathe for natural detox. Call ChiroMed in El Paso, TX, to book—your gut will thank you.
Unlock the potential of chiropractic care for pain management and improved physical well-being from disc herniation and disc bulging.
Understanding Disc Herniation and Disc Bulging: A Comprehensive Clinical Guide to Chiropractic Care and Spinal Decompression
Unlocking the Path to Recovery: Evidence-Based Chiropractic Solutions for Spinal Disc Disorders
According to Al Qaraghli and De Jesus (2023), back pain is one of the most common health issues impacting contemporary society, with 80% of people suffering at least one episode throughout their lifetime. Two of the most prevalent—yet usually misdiagnosed—causes of incapacitating pain among this wide range of spinal disorders are disc herniation and disc bulging. Understanding the clinical differences between neck, mid-back, and lower back pain, and the available evidence-based treatment options, especially chiropractic care and nonsurgical spinal decompression therapy, can help patients experiencing chronic pain radiating through these regions find long-lasting relief and functional restoration.
Understanding the Spinal Disc: Anatomy and Function
The human spine is a marvel of biological engineering, consisting of 24 vertebrae stacked on one another, separated by intervertebral discs that serve as sophisticated shock absorbers. These discs play multiple essential roles: they maintain height between vertebrae, absorb mechanical forces during movement and impact, facilitate spinal flexibility, and distribute biomechanical loads evenly throughout the spinal column (Al Qaraghli & De Jesus, 2023). Each intervertebral disc comprises two distinct structural components. The annulus fibrosus forms the tough, circular outer portion composed of 15 to 25 stacked sheets of highly organized fibrous connective tissue, predominantly type 1 collagen in the outer layers and type 2 collagen in the inner portions. Surrounding this protective shell lies the nucleus pulposus, a gel-like inner core consisting of a loose network of fibers suspended in a hydrophilic matrix. At birth, approximately 80% of disc composition consists of water, and proper hydration remains essential for optimal disc function throughout life (El Paso Chiropractor Blog, 2016). The structural integrity of healthy discs has often been compared to a jelly doughnut—a resilient outer ring containing a soft, gelatinous center. This unique composition enables discs to evenly distribute forces and pressures applied to the spine during daily activities, maintaining spinal stability while permitting controlled movement.
Disc Herniation vs. Disc Bulging: Critical Distinctions and Similarities
While disc herniation and disc bulging both involve displacement of disc material beyond normal anatomical boundaries, understanding their fundamental differences proves critical for appropriate clinical management and patient education.
Disc Bulging: Contained Disc Displacement
A disc bulge (also termed disc prolapse) occurs when the nucleus pulposus presses against the annulus fibrosus wall, causing the disc to protrude outward beyond its usual borders. Critically, in a bulging disc, the outer annular fibers remain intact—the gel-like nucleus stays fully contained within the disc structure, even though the entire disc extends beyond its normal space (Mayo Clinic, 2024). This condition typically affects at least 25% to 50% of the disc’s circumference and involves only the outer layer of tough cartilage (El Paso Chiropractor Blog, 2016).
The bulging disc can still compress surrounding neural structures, including spinal nerves and the spinal cord, potentially causing pain, numbness, tingling, and functional limitations. However, because the disc material remains contained, symptoms are often milder than with herniated discs, unless significant nerve compression occurs (Neurosurgery One, 2025).
Disc Herniation: Rupture and Extrusion
In contrast, a disc herniation (also called disc extrusion, ruptured disc, or slipped disc) develops when the tough outer annulus fibrosus develops a crack or tear, allowing the soft nucleus pulposus to squeeze through the opening and protrude into the spinal canal (Mayo Clinic, 2024). The herniated material can spread to adjacent structures, including the spinal cord and spinal nerve roots, often compressing these delicate tissues and triggering a cascade of symptoms (El Paso Chiropractor Blog, 2016).
When disc material herniates, two distinct pathological mechanisms contribute to pain generation. First, mechanical compression of neural structures directly irritates and damages nerve tissue. Second, the chemical composition of the nucleus pulposus itself proves highly inflammatory—when exposed to the immune system, these materials trigger significant inflammatory responses characterized by swelling, pain, and immune cell infiltration (Cosamalón-Gan et al., 2021).
Similarities Between Disc Conditions
Despite their structural differences, disc herniation and disc bulging share several important characteristics:
Common Symptom Patterns: Both conditions can produce identical or nearly identical symptoms, including localized back or neck pain, radiating pain into extremities (radiculopathy), numbness and tingling sensations, muscle weakness, and limited range of motion (Neurosurgeons of New Jersey, 2023).
Age-Related Degeneration: Both conditions typically arise from the spine’s natural degenerative process. As individuals age, spinal discs progressively dehydrate, becoming stiffer, more fragile, and less capable of adjusting to compression and mechanical stress. This degeneration represents the primary underlying cause for most disc complications (El Paso Chiropractor Blog, 2016).
Nerve Compression Mechanisms: Whether bulging or herniated, displaced disc material can impinge on spinal nerve roots or the spinal cord, triggering nerve irritation, inflammation, and the characteristic pain patterns associated with these conditions (Al Qaraghli & De Jesus, 2023).
Asymptomatic Presentations: Remarkably, many individuals harbor disc bulges or herniations without experiencing any symptoms whatsoever. These conditions are frequently discovered incidentally during imaging studies performed for unrelated medical issues (Mayo Clinic, 2024).
Regional Manifestations: How Disc Disorders Affect the Cervical, Thoracic, and Lumbar Spine
Disc herniation and bulging can develop throughout the spinal column, though certain regions are more vulnerable. The clinical presentation, symptom patterns, and functional impairments vary significantly depending on the spinal region affected.
Cervical Spine Disc Disorders
The cervical spine, comprising seven vertebrae in the neck, is the second most common site of symptomatic disc herniation. The most frequently affected levels are C4-C5, C5-C6, and C6-C7, with C6-C7 most likely to herniate in the cervical region (Spine-health, 2019).
Clinical Manifestations: Cervical disc herniation typically produces neck pain located toward the back or side of the neck, ranging from mild tenderness to sharp, burning sensations (Spine-health, 2019). Radicular pain—characterized by electric shock-like or hot sensations—commonly radiates from the neck down through the shoulder, arm, hand, and fingers. The specific distribution of symptoms depends on which nerve root suffers compression:
C5 nerve root (C4-C5 herniation): Pain and tingling radiating to the shoulder, with potential weakness in the deltoid muscle
C6 nerve root (C5-C6 herniation): Pain, tingling, and numbness affecting the thumb side of the hand, with weakness in the biceps and wrist extensors
C7 nerve root (C6-C7 herniation): Symptoms extending to the middle finger, with triceps weakness and finger extensor dysfunction
C8 nerve root (C7-T1 herniation): Pain and numbness in the pinky side of the hand, with handgrip weakness
Cervical herniated discs can also trigger cervical myelopathy when disc material compresses the spinal cord itself. This serious condition produces bilateral symptoms including numbness, weakness, balance disturbances (ataxia), hyperreflexia, and potential urinary incontinence. Chronic myelopathy may progress insidiously, sometimes delaying diagnosis as patients attribute symptoms to normal aging (Kamran Aghayev, 2025).
Thoracic Spine Disc Disorders
Thoracic disc herniations represent the rarest form of symptomatic disc pathology, with an estimated incidence of approximately one in one million per year, accounting for only 0.25% to 0.75% of total symptomatic spinal disc herniations (BCMJ, 2019). Despite this rarity, thoracic disc disorders present unique diagnostic challenges due to their atypical symptom presentations.
Clinical Manifestations: Thoracic herniated discs produce three distinct clinical patterns (Barrow Neurological Institute, 2025):
Radiculopathy (affecting approximately 52% of symptomatic patients): Mid-back pain that may wrap around the chest in a band-like distribution, corresponding to the dermatomal pattern of the affected nerve root. Patients often describe sensations of a strap tightening around their chest. Pain may also manifest as numbness, pressure sensations, or generalized discomfort rather than classic pain.
Myelopathy (affecting approximately 70% of symptomatic patients): Spinal cord compression producing difficulty walking, progressive lower extremity weakness and numbness, wide-based gait, increased muscle tone and clonus, hyperreflexia in lower extremities, and occasional bowel dysfunction.
Atypical extraspinal symptoms: Thoracic disc herniations frequently produce misleading symptoms, including nausea, emesis, chest tightness, gastrointestinal complaints, chronic constipation, buttock and leg burning pain, and urinary frequency—often leading to extensive workups for cardiac, pulmonary, or gastrointestinal disorders before the correct diagnosis emerges (Physio-pedia, 2023).
The most commonly affected thoracic levels include T7-T8, T8-T9, and T11-T12, with disc pathologies identified in approximately 18% of thoracic intervertebral disc levels among symptomatic patients (Turkish Journal of Medical Sciences, 2019).
Lumbar Spine Disc Disorders
The lumbar spine represents the most common location for disc herniation and bulging, with approximately 95% of lumbar disc herniations occurring at the L4-L5 or L5-S1 levels. Lumbar disc herniation affects 5 to 20 individuals per 1,000 adults annually, with peak prevalence occurring in the third to fifth decades of life and a male-to-female ratio of 2:1 (Al Qaraghli & De Jesus, 2023).
Clinical Manifestations: Lumbar disc disorders typically produce:
Low back pain: The primary symptom, arising from pressure exerted by herniated disc material on the posterior longitudinal ligament and local inflammation. The pain is often mechanical, worsening with movement, prolonged sitting, straining, coughing, and sneezing (Al Qaraghli & De Jesus, 2023).
Radiculopathy (sciatica): When disc material compresses lumbar nerve roots, pain radiates into the buttocks, thighs, calves, and feet, following specific dermatomal patterns:
L4 nerve root (L4-L5 herniation): Pain radiating to the anterior thigh and medial leg, with weakness in hip flexion/adduction and knee extension, plus diminished patellar reflex
L5 nerve root (L5-S1 herniation): Pain extending to the buttock, lateral thigh, lateral calf, dorsum of foot, and great toe, with weakness in foot dorsiflexion, great toe extension, and foot inversion/eversion
S1 nerve root (S1-S2 herniation): Sacral/buttock pain radiating to the posterolateral thigh, calf, and lateral/plantar foot, with weakness in plantar flexion and diminished Achilles reflex
Neurological deficits —sensory abnormalities (numbness, tingling), motor weakness, muscle atrophy in chronic cases, and altered reflexes — characterize nerve root compression. Severe central herniations may produce cauda equina syndrome, a surgical emergency characterized by saddle anesthesia, bowel/bladder incontinence, and progressive bilateral lower extremity weakness (Al Qaraghli & De Jesus, 2023).
Environmental and Occupational Risk Factors: Creating Overlapping Risk Profiles for Back Pain
While genetic factors contribute significantly to disc degeneration and herniation susceptibility, environmental and occupational exposures create substantial additional risk, often producing overlapping risk profiles that compound individual vulnerability to back pain across all spinal regions.
Occupational Physical Demands
Heavy physical workload and occupations requiring strenuous effort are associated most strongly with lumbar disc herniation risk. Research examining risk factors for lumbar disc herniation with radiculopathy identified occupation—particularly heavy labor—among the most robust risk factors, with certain professions showing risk ratios up to 6.0 (Dynamic Disc Designs, 2024).
Specific occupational activities that increase disc herniation risk include:
Repetitive lifting, bending, and twisting: Cumulative exposure to lifting heavy weights, forward bending, and rotational movements significantly increases lumbar disc herniation risk (Risk Factors Study, 2021)
Prolonged sitting: Sedentary work increases the risk of disc degeneration by exerting sustained compression loads on the spine during extended sitting. Sitting increases intradiscal pressure by approximately 40% compared to standing, intensifying mechanical stress on already vulnerable discs (Al Qaraghli & De Jesus, 2023)
Extended work hours: Working periods exceeding 8 hours consistently and experiencing high workplace stress levels are both associated with elevated disc herniation risk (Spine-health, 2024)
Whole-body vibration: Occupations involving prolonged exposure to vibration (truck drivers, heavy equipment operators) accelerate disc degeneration
Built Environment and Healthy Building Determinants
Emerging evidence indicates that indoor environmental quality and healthy building determinants significantly influence the risk of back and neck pain. A systematic review examining relationships between healthy building determinants and back/neck pain found evidence generally supporting that as healthy building determinants worsen—including poor air quality, inadequate ventilation, dust exposure, suboptimal lighting, moisture problems, excessive noise, thermal discomfort, and poor water quality—the risk of back and neck pain increases (PMC, 2022).
Given that people spend more than 90% of their time indoors, the built environment where most back and neck pain episodes occur deserves greater attention in prevention strategies. Poor environmental factors, including noise, dust, gases, fumes, and poor air quality, were significantly associated with increased back pain risk in both men and women across multiple studies (PMC, 2022).
Age and degeneration: While aging itself remains unavoidable, the natural degenerative cascade—characterized by reduced water content, increased type 1 collagen ratios in the nucleus pulposus, destruction of extracellular matrix, and upregulated inflammatory pathways—progresses throughout adult life, with disc herniation most prevalent between ages 30-50 (Al Qaraghli & De Jesus, 2023).
Obesity and excess weight: Elevated body mass index dramatically increases disc herniation risk by placing excessive mechanical load on the spine, accelerating disc degeneration and making herniation more likely. Excess body fat, particularly around the chest and abdomen, intensifies biomechanical stress on the lower back while promoting systemic inflammation (Spine-health, 2024).
Nicotine use: Smoking, vaping, and tobacco chewing disrupt nutrient flow to intervertebral discs, inhibit nucleus pulposus cell growth, and reduce collagen synthesis—all accelerating disc degeneration (Spine-health, 2024).
Sedentary lifestyle: Physical inactivity leads to weak core muscles, poor posture, and reduced flexibility, all of which increase stress on spinal discs. Regular low-impact exercise strengthens muscles supporting the spine and improves overall spinal health (Leucadia Chiropractic, 2025).
Improper lifting techniques: Using the back instead of legs when lifting, twisting while lifting, or attempting to carry excessive weight places dangerous pressure on the spine, potentially triggering acute herniation in susceptible individuals.
Cardiovascular risk factors: Surprisingly, high cholesterol, hypertension, diabetes, and family history of coronary disease all associate with higher lumbar disc herniation risk, particularly in women, suggesting metabolic health plays important roles in disc pathology (Dynamic Disc Designs, 2024).
Genetic Susceptibility and Gene-Environment Interactions
Twin studies demonstrate that both genetic and environmental factors contribute substantially to disc degeneration and back pain. Genetic factors appear to influence disc narrowing and degeneration—key pathways through which genes influence the development of back pain (FYZICAL, 2006). However, environmental factors interact with genetic predisposition, creating complex risk profiles where occupational exposures, lifestyle choices, and built environment quality either amplify or mitigate underlying genetic vulnerability.
Research on Finnish twins revealed that approximately 41% of the total variance in childhood low back pain could be attributed to shared environmental factors within families, while 59% stemmed from unique environmental factors, with genetic factors playing at most a minor role in pediatric populations (PMC, 2008). This underscores the critical importance of identifying and modifying environmental risk factors to prevent disc pathology across the lifespan.
The Inflammatory Cascade: Biochemical Mediators of Disc-Related Pain
Understanding disc herniation requires moving beyond purely mechanical models of nerve compression to appreciate the complex inflammatory processes that amplify and perpetuate pain. Until fairly recently, sciatic pain and radiculopathy associated with lumbar disc herniation were attributed exclusively to mechanical compression of nerve roots. However, mounting evidence from immunology, immunohistochemistry, and molecular biology studies indicates that herniated disc tissue is biologically active, expressing numerous inflammatory mediators that play central roles in pain generation (Cosamalón-Gan et al., 2021).
Pro-Inflammatory Cytokines
Herniated and degenerated discs demonstrate markedly elevated levels of pro-inflammatory cytokines, including:
Interleukin-1 beta (IL-1β): A master regulator of inflammatory responses that stimulates production of matrix metalloproteinases (MMPs), promoting extracellular matrix breakdown and disc degeneration. IL-1β also induces expression of additional inflammatory mediators and chemokines (PMC, 2013).
Tumor Necrosis Factor-alpha (TNF-α): Works synergistically with IL-1β to promote matrix degradation, increase production of catabolic enzymes, and stimulate inflammatory pathways. TNF-α directly sensitizes nociceptors, lowering pain thresholds and increasing pain sensitivity (PMC, 2013).
Interleukin-6 (IL-6): Elevated in degenerated and herniated discs, IL-6 contributes to chronic inflammatory states and correlates with pain intensity. Recent research demonstrates that disc herniation severity associates with circulating IL-6 levels, with this relationship particularly pronounced in patients with chronic symptoms (NYP Advances, 2020).
Interleukin-8 (IL-8): A potent chemotactic factor that recruits neutrophils to sites of disc herniation. Co-neutralization of IL-8 and TNF-α significantly improved mechanical hyperalgesia in experimental models (PMC, 2013).
Interleukin-17 (IL-17): Plays important roles in recruiting T-cells and macrophages and activating glial and astrocytic cells during nerve injury and subsequent neuropathic pain. IL-17 levels show significant elevation in herniated versus merely degenerated discs (PMC, 2013).
Chemokines and Immune Cell Recruitment
Beyond structural damage, inflammatory cytokines stimulate disc cells to produce chemotactic factors that recruit immune cells—including macrophages, neutrophils, and T cells—to the disc and surrounding tissues. Analysis of herniated discs reveals elevated levels of multiple chemokines, including:
Monocyte chemotactic protein-1 (MCP-1, CCL2)
CCL3, CCL4, CCL5
MCP-3, MCP-4
CXCL10
Expression of CCL3 correlates positively with degeneration grade and is higher in herniated tissue compared with degenerate but contained discs. By regulating chemokine expression, inflammatory cytokines promote C-C chemokine receptor type 1 (CCR1)-dependent macrophage migration, thereby establishing a self-perpetuating inflammatory cycle critical to pain-generating pathways (PMC, 2013).
Autoimmune Responses
Inflammation in disc herniation stems not only from chemical irritation by bioactive substances released from the nucleus pulposus but also from autoimmune responses against disc tissue itself. The nucleus pulposus, normally sequestered from the immune system, becomes recognized as foreign when herniation exposes it to immune surveillance. This triggers antibody production and T-cell-mediated responses that amplify local inflammation (Cosamalón-Gan et al., 2021).
Clinical Implications of Inflammatory Mechanisms
This biochemical understanding carries profound clinical implications. First, it explains why some patients experience severe pain despite relatively minor disc herniations—individual variations in inflammatory responses may prove more important than herniation size alone. Second, it validates treatment approaches targeting inflammation, including judicious use of anti-inflammatory medications and interventions like epidural steroid injections. Third, it suggests that therapies that promote the resolution of inflammation and support tissue healing—such as chiropractic care and spinal decompression—may address root causes rather than merely manage symptoms.
Clinical Rationale for Chiropractic Care in Disc Herniation and Bulging
Chiropractic care has emerged as a primary conservative treatment modality for patients suffering from disc herniation and bulge, supported by growing evidence demonstrating significant clinical benefits. The clinical rationale for chiropractic intervention in disc pathology rests on multiple therapeutic mechanisms that address both mechanical dysfunction and inflammatory processes.
Mechanisms of Chiropractic Spinal Manipulation
Chiropractic spinal manipulation—characterized by high-velocity, low-amplitude (HVLA) controlled forces applied to specific spinal segments—produces multiple beneficial effects in patients with disc disorders:
Restoration of spinal alignment and mobility: Spinal manipulation corrects vertebral misalignments (subluxations) that may contribute to abnormal biomechanical stress on intervertebral discs. By restoring proper spinal alignment, manipulation reduces asymmetric loading that accelerates disc degeneration (El Paso Chiropractor Blog, 2016).
Reduction of intradiscal pressure: Properly executed spinal manipulation may temporarily reduce pressure within affected discs, potentially facilitating retraction of herniated material and reducing compression on adjacent neural structures.
Improvement of spinal joint function: Manipulation increases range of motion in restricted spinal segments, reducing mechanical irritation of surrounding tissues and improving overall spinal biomechanics.
Modulation of pain perception: Spinal manipulation activates mechanoreceptors and produces neurophysiological effects that may modulate pain perception via gate-control mechanisms and descending pain-inhibition pathways.
Anti-inflammatory effects: Emerging evidence suggests that spinal manipulation may influence inflammatory processes, potentially reducing local cytokine production and promoting the resolution of inflammation.
Clinical Outcomes Evidence for Chiropractic Care
Multiple high-quality studies document the effectiveness of chiropractic spinal manipulation for disc herniation and bulging across spinal regions:
Lumbar Disc Herniation: A landmark prospective cohort study published in the Journal of Manipulative and Physiological Therapeutics followed 148 patients aged 18-65 with low back pain, leg pain, and MRI-confirmed lumbar disc herniation treated with high-velocity, low-amplitude spinal manipulation (Leemann et al., 2014). Outcomes proved remarkable:
At 3 months, 90.5% of patients reported “improvement” on global impression of change scales
At 1 year, 88.0% maintained “improved” status
Among chronic patients (symptoms >3 months), 81.8% reported improvement, increasing to 89.2% at 1 year
Both acute and chronic patients demonstrated significant improvements in numerical rating scale scores for low back pain, leg pain, and Oswestry Disability Index scores at all follow-up points (2 weeks, 1, 3, 6, and 12 months)
No adverse events were reported throughout the study period
The high success rates among chronic patients are particularly noteworthy, as this population typically shows poorer responses to conservative interventions. The sustained improvements at one-year follow-up indicate that chiropractic manipulation produces lasting benefits rather than merely temporary symptom relief.
Cervical Disc Herniation: Research from Zurich, Switzerland, examined 50 patients aged 18-65 with MRI-confirmed cervical disc herniation treated with chiropractic spinal manipulation at frequencies of 3-5 sessions weekly initially, reducing to 1-3 sessions weekly until symptom resolution (SSPT Chiropractic, 2024). Results demonstrated progressive improvement:
At 2 weeks, 55% of participants reported improvement
At 1 month, 68.8% showed improvement
At 3 months, 85.4% experienced favorable outcomes
Even among chronic cervical disc herniation patients, 76% reported beneficial effects, including reduced neck and arm pain
Another study specifically examining patients with MRI-confirmed lumbar disc herniation and concomitant sacroiliac joint hypomobility found that five sessions of lumbar and sacroiliac joint manipulation over a 2-week period produced significant improvements in both back and leg pain intensity and functional disability, as measured by the Oswestry Disability Index (Shokri et al., 2018).
Comparative Effectiveness: Research comparing chiropractic spinal manipulative therapy (CSMT) with other care modalities for newly diagnosed lumbar disc herniation and lumbar spinal radiculopathy found that patients receiving CSMT demonstrated significantly reduced odds of requiring lumbar discectomy surgery through 2-year follow-up compared to those receiving other care approaches (BMJ Open, 2022). This suggests that chiropractic care may help many patients avoid surgical intervention while achieving satisfactory functional outcomes.
Dr. Alexander Jimenez’s Integrative Approach
Dr. Alexander Jimenez, DC, APRN, FNP-BC, exemplifies the modern integrative chiropractic practitioner, combining advanced clinical expertise with comprehensive diagnostic evaluation to optimize patient outcomes. As both a board-certified Doctor of Chiropractic and Family Practice Nurse Practitioner practicing in El Paso, Texas, Dr. Jimenez brings a unique dual-scope perspective to treating complex spinal disorders, including disc herniation and bulging. Dr. Jimenez’s clinical approach emphasizes thorough diagnostic evaluation utilizing advanced imaging modalities—including MRI and other radiological studies—to precisely characterize disc pathology before initiating treatment. This imaging-guided approach ensures that manipulation techniques are appropriately tailored to each patient’s specific disc lesion type, location, and severity. As noted on his clinical website (dralexjimenez.com), Dr. Jimenez focuses on treating patients with “complex herniated discs” using evidence-based protocols that integrate chiropractic manipulation, functional medicine principles, nutritional optimization, and rehabilitation exercises. His dual training enables comprehensive evaluation of patients from both musculoskeletal and medical perspectives, identifying underlying metabolic, inflammatory, or systemic factors that may contribute to disc degeneration and impaired healing. Dr. Jimenez emphasizes that proper patient selection proves critical—when patients present with conditions better suited for alternative treatments or specialist referral, he ensures they receive appropriate care from the most qualified providers. The integration of functional medicine assessment tools, including detailed evaluations of genetics, lifestyle factors, environmental exposures, nutritional status, and psychological/emotional factors, enables Dr. Jimenez to address the root causes of disc pathology rather than merely treating symptoms. This comprehensive approach aligns with emerging evidence demonstrating that metabolic health, inflammatory status, and environmental factors significantly influence disc degeneration progression and healing potential.
Spinal Decompression in Depth- Video
Nonsurgical Spinal Decompression: Mechanism, Evidence, and Clinical Application
Nonsurgical spinal decompression therapy (NSDT) represents an advanced evolution of traditional traction therapy, utilizing sophisticated computer-controlled systems to create negative intradiscal pressure that facilitates disc healing and symptom resolution. Understanding the distinctions between NSDT and conventional traction proves essential for appreciating this intervention’s unique therapeutic potential.
Mechanism of Action: Creating Negative Intradiscal Pressure
NSDT operates through a precisely controlled biomechanical process fundamentally different from traditional traction:
Specialized positioning: Patients are positioned on a computer-controlled decompression table with the spine properly aligned and supported. Harnesses secure the upper body (chest and shoulders) while a separate harness attaches to the pelvis or lower body.
Computer-guided distraction: Unlike conventional traction that applies a constant pulling force, NSDT employs a sophisticated algorithm that gradually increases and decreases distraction force in cyclical patterns. This intermittent loading prevents reflexive muscle guarding, which limits the effectiveness of traditional traction (Hill DT Solutions, 2024).
Negative intradiscal pressure generation: The controlled distraction force creates a vacuum effect within targeted intervertebral discs. Research measuring intradiscal pressure during NSDT using pressure transducers inserted into the L4-L5 disc space demonstrated that decompression therapy can lower pressure in the nucleus pulposus to below -100 mmHg, compared to standard progressive traction achieving only -40 mmHg (compared to -75 mmHg resting supine) (Hill DT Solutions, 2024).
Disc material retraction: This sustained negative pressure may facilitate retraction of herniated or bulging nucleus pulposus material away from compressed neural structures. The vacuum effect theoretically “pulls” extruded disc material back toward its normal position within the disc space.
Enhanced nutrient influx: Negative intradiscal pressure promotes increased fluid exchange, drawing oxygen, nutrients, and hydration into degenerated discs. This enhanced nutrient delivery may support disc cell metabolism and tissue repair (Dr. DiGrado, 2024).
Spinal joint decompression: The distraction force increases the width of the intervertebral foramen, reducing pressure on exiting nerve roots and facet joints, thereby contributing to pain relief independent of effects on the disc itself.
Critical Distinction from Traditional Traction
The fundamental advantage of NSDT over conventional traction lies in its ability to overcome the muscle guarding reflex. When traditional traction applies sudden or sustained pulling forces, paraspinal muscles reflexively contract to protect the spine from perceived threat. This muscle contraction increases internal disc pressure and limits the therapeutic effect (Choi et al., 2022).NSDT systems employ gradual force application with intermittent relaxation phases that prevent this protective muscle contraction. The computer continuously monitors resistance and adjusts force application in real time, maintaining the spine in a relaxed state while delivering far greater decompressive forces than traditional traction can achieve. This creates what researchers describe as a “zero-gravitation” state in targeted discs (Choi et al., 2022).
Evidence for NSDT Effectiveness
A rigorous randomized controlled trial published in the International Journal of Clinical Practice provides compelling evidence for the effectiveness of NSDT in treating subacute lumbar disc herniation (Choi et al., 2022). This study enrolled 60 patients with subacute lumbar herniated intervertebral disc, randomizing them to either:
Decompression group (n=30): Received 10 NSDT sessions over 8 weeks (twice weekly for 2 weeks, then once weekly for 6 weeks), with distraction force starting at half body weight minus 5 kg and increasing by 1 kg per session
Nondecompression group (n=30): Received identical positioning and session frequency but with zero distraction force (sham treatment)
Results demonstrated significant advantages for the decompression group:
Pain outcomes:
Lower leg pain intensity at 2 months (p=0.028)
Significant reductions in low back and leg pain from baseline to 3 months in both groups (p<0.001), though between-group differences in back pain did not reach significance
Functional outcomes:
Significantly lower Korean Oswestry Disability Index scores at 2 months (p=0.023) and 3 months (p=0.019)
MRI-documented structural changes:
Herniation index decreased by 27.6±27.5% in the decompression group versus only 7.1±24.9% in the control group (p=0.017)
26.9% of decompression patients versus 0% of control patients achieved >50% reduction in herniation index (p=0.031)
42.3% of decompression patients achieved ≥30% herniation reduction versus 17.6% of controls
These findings prove groundbreaking—this study represents the first randomized controlled trial to document that NSDT produces measurable reductions in disc herniation volume as confirmed by follow-up MRI, while simultaneously improving pain and function. The fact that actual structural healing occurred rather than merely symptomatic improvement suggests that NSDT addresses the underlying pathology. Additional research supports these findings. A retrospective cohort study examining adults with chronic low back pain attributed to disc herniation or discogenic pain who underwent 6-week NSDT protocols via the DRX9000 system found significant correlations between disc height restoration and pain reduction (Apfel et al., 2010). Low back pain decreased from 6.2±2.2 to 1.6±2.3 (p<0.001) while disc height increased from 7.5±1.7mm to 8.8±1.7mm (p<0.001), with these variables showing significant correlation (r=0.36, p=0.044). Long-term follow-up studies demonstrate sustained benefits. Research tracking patients 4 years after completing NSDT protocols found that 52% maintained pain levels of zero, 91% resumed normal daily activities, and over 80% achieved 50% or greater pain reduction compared to pre-treatment baselines (Pain Free Charleston, 2004).
NSDT Treatment Protocols
Typical NSDT treatment courses involve:
Session frequency: 10-20 sessions over 4-8 weeks, with initial sessions typically scheduled 2-3 times weekly, reducing to 1-2 times weekly as improvement occurs
Session duration: 20-30 minutes per session
Force parameters: Distraction force is individualized based on patient body weight, disc level targeted, and tolerance, typically starting at conservative levels (40-50% body weight) and gradually progressing
Positioning: Supine positioning with flexed knees for lumbar protocols; prone or supine with cervical harness for cervical protocols
Cycle patterns: Alternating distraction and relaxation phases (commonly 60 seconds of tension, 30 seconds of relaxation) to prevent muscle guarding
Adjunctive therapies: Many protocols combine NSDT with complementary treatments, including cold/heat therapy, electrical stimulation, therapeutic exercise, and nutritional support to optimize outcomes
Safety and Contraindications
NSDT demonstrates excellent safety profiles when appropriately applied. The randomized controlled trial by Choi and colleagues reported zero adverse events throughout the study period (Choi et al., 2022). Similarly, the large prospective cohort study by Leemann and colleagues involving 148 patients receiving chiropractic manipulation for MRI-confirmed disc herniation reported no adverse events (Leemann et al., 2014).
However, certain contraindications to NSDT must be respected:
Absolute contraindications:
Pregnancy
Fracture
Tumor
Abdominal aortic aneurysm
Advanced osteoporosis
Cauda equina syndrome requiring emergency surgery
Severe spinal instability
Relative contraindications:
Prior spinal surgery with hardware
Severe disc degeneration with >50% height loss
Sequestrated disc fragments
Severe spinal stenosis
Extreme obesity is limiting proper positioning
Proper patient selection, thorough clinical examination, and careful review of imaging studies by qualified practitioners ensure NSDT is applied to appropriate candidates while avoiding potential complications.
Integrating Chiropractic Care and Spinal Decompression: Complementary Approaches
For many patients with disc herniation and bulging, optimal outcomes emerge from integrating multiple conservative therapies rather than relying on single interventions. Chiropractic spinal manipulation and NSDT offer complementary mechanisms that address different aspects of disc pathology:
Chiropractic manipulation primarily restores spinal joint mobility, corrects vertebral misalignments, modulates pain through neurophysiological mechanisms, and may influence local inflammatory processes. It proves particularly effective for acute presentations and when joint dysfunction accompanies disc pathology.
NSDT specifically targets the disc itself, creating negative intradiscal pressure that facilitates disc material retraction, promotes nutrient influx, and directly decompresses neural structures. It excels in cases where significant disc herniation or advanced degeneration requires sustained decompressive forces.
When combined, these approaches provide:
Comprehensive address of both joint dysfunction and disc pathology
Multiple mechanisms for pain relief and functional restoration
Options for tailoring treatment intensity to individual patient tolerance
Complementary effects that may accelerate healing beyond either therapy alone
Dr. Jimenez’s integrative approach exemplifies this comprehensive strategy, combining chiropractic adjustments with spinal decompression, functional medicine interventions, nutritional optimization, therapeutic exercise, and patient education to address all contributors to disc pathology and optimize healing potential.
Patient Selection and Prognostic Factors
Not all patients with disc herniation or bulging require or benefit equally from chiropractic care and spinal decompression. Understanding prognostic factors helps identify ideal candidates:
Favorable prognostic indicators:
Acute to subacute symptom duration (4 weeks to 3 months)
First episode of disc-related pain
Absence of progressive neurological deficits
Contained disc herniations (protrusions, extrusions) rather than sequestrations
Younger age (generally <65 years)
Absence of significant comorbidities
High motivation and compliance with treatment protocols
Adequate disc height preservation on imaging
Factors suggesting need for alternative or adjunctive interventions:
Significant psychological distress or catastrophizing
Major comorbidities affecting healing capacity
Even among chronic patients, evidence suggests substantial benefit from chiropractic care and NSDT, with the Leemann study demonstrating 89.2% of chronic lumbar disc herniation patients reporting improvement at 1-year follow-up after chiropractic manipulation (Leemann et al., 2014).
Conclusion: Evidence-Based Hope for Disc Pathology
The evidence presented in this extensive review leads to an unequivocal conclusion: chiropractic care and nonsurgical spinal decompression therapy are evidence-based and effective treatment modalities for patients with disc herniation and disc bulging in the cervical, thoracic, and lumbar spine regions. For patients enduring the debilitating pain, functional limitations, and quality-of-life impairments linked to disc pathology, these conservative interventions present hope based on robust scientific evidence. Studies consistently show that carefully selected patients who receive chiropractic spinal manipulation experience clinically significant improvements in pain, disability, and overall function. Depending on the patient’s characteristics and outcome measures, the success rates range from 76% to over 90%. Incredibly, these benefits last, as shown by follow-ups one year later and beyond. NSDT adds a powerful tool that can make measurable structural changes, such as a real decrease in disc herniation volume confirmed by MRI, as well as relieve symptoms. The capacity to record disc healing, rather than solely symptom management, signifies a transformative advancement in conservative disc care. The clinical insights from practitioners such as Dr. Alexander Jimenez, DC, APRN, FNP-BC, who combine advanced diagnostic evaluation, dual-scope clinical expertise, and comprehensive treatment protocols, show how modern chiropractic practice has moved beyond the limits of the past. Integrative approaches address the root causes of disc pathology while supporting the body’s natural healing abilities by combining spinal manipulation, decompression therapy, functional medicine principles, nutritional optimization, and patient education. Environmental and occupational risk factors generate overlapping vulnerability profiles that exacerbate genetic predisposition to disc degeneration. Recognizing these modifiable factors—such as workplace ergonomics, physical demands, built environment quality, obesity, smoking, sedentary lifestyle, and metabolic health—facilitates comprehensive prevention and treatment strategies that transcend mere symptom management. Understanding the inflammatory cascade that causes disc-related pain, which involves complex interactions among pro-inflammatory cytokines, chemokines, immune cell infiltration, and autoimmune responses, provides a mechanistic rationale for treatments that focus on reducing inflammation and healing tissue rather than just blocking pain signals. The evidence examined here provides genuine hope for significant recovery for the millions of individuals experiencing disc-related back and neck pain through conservative, nonsurgical approaches. Not every patient will achieve total resolution, and some may ultimately necessitate surgical intervention; however, the vast majority can anticipate considerable improvement through appropriately administered chiropractic care and spinal decompression therapy.
Important Medical Disclaimer and Serious Note to Readers
THIS ARTICLE IS INTENDED FOR INFORMATIONAL AND EDUCATIONAL PURPOSES ONLY AND SHOULD NOT BE CONSTRUED AS MEDICAL ADVICE, DIAGNOSIS, OR TREATMENT RECOMMENDATION.
The information presented in this article, while based on peer-reviewed scientific literature and clinical evidence, does not substitute for professional medical evaluation, diagnosis, and treatment. Disc herniation, disc bulging, and related spinal conditions can produce serious complications, including permanent neurological damage, paralysis, bowel and bladder dysfunction, and chronic pain syndromes if inappropriately managed.
DO NOT ATTEMPT TO SELF-DIAGNOSE OR SELF-TREAT DISC-RELATED CONDITIONS. If you are experiencing back pain, neck pain, radiating pain into extremities, numbness, tingling, weakness, or any other symptoms potentially related to spinal disc pathology, seek immediate evaluation from qualified healthcare professionals.
CERTAIN SYMPTOMS CONSTITUTE MEDICAL EMERGENCIES requiring immediate emergency department evaluation, including:
Sudden onset of bowel or bladder incontinence or retention
Progressive lower extremity weakness or paralysis
Saddle anesthesia (numbness in the groin/inner thigh region)
Severe pain unresponsive to conservative measures
Symptoms following significant trauma
Chiropractic care and spinal decompression therapy, while generally safe when appropriately applied, carry potential risks and contraindications. These interventions should be performed only by licensed, qualified practitioners after thorough clinical examination and review of appropriate imaging studies. Improper application of spinal manipulation or decompression therapy can potentially worsen disc herniation, cause neurological damage, or result in other serious complications. The treatment outcomes and success rates cited in this article represent average findings from clinical studies and should not be interpreted as guarantees of individual outcomes. Individual results vary based on numerous factors, including age, overall health status, severity and duration of disc pathology, presence of comorbidities, lifestyle factors, and compliance with treatment protocols.
Before initiating any treatment for disc-related conditions, patients should:
Undergo a comprehensive evaluation by qualified healthcare providers
Obtain appropriate imaging studies (MRI, CT, or X-ray as indicated)
Discuss all treatment options, including risks, benefits, and alternatives
Ensure practitioners are properly licensed and credentialed
Verify that their specific condition is appropriate for conservative management
Understand when surgical intervention may be necessary
References to Dr. Alexander Jimenez and his clinical approaches are provided for illustrative purposes, demonstrating integrative treatment models and should not be construed as specific endorsements or treatment recommendations. Patients seeking care should independently research practitioners’ credentials, experience, and patient outcomes. The authors and publishers of this article disclaim all liability for any adverse outcomes, complications, or damages resulting from the application of information contained herein. Readers assume all responsibility and risk for decisions made regarding their healthcare and treatment choices. This article addresses complex medical conditions requiring individualized assessment and treatment planning. What proves safe and effective for one patient may be inappropriate or dangerous for another. Always consult qualified healthcare professionals for personalized medical advice specific to your individual circumstances. If you are currently experiencing a medical emergency, call emergency services (911 in the United States) immediately. Do not delay seeking emergency care while researching conservative treatment options. By continuing to read and apply information from this article, you acknowledge understanding and accepting this disclaimer and assume full responsibility for your healthcare decisions.
Apfel, C. C., Cakmakkaya, O. S., Martin, W., Richmond, C., Macario, A., George, E., Schaefer, M., & Pergolizzi, J. V. (2010). Restoration of disk height through non-surgical spinal decompression is associated with decreased discogenic low back pain: A retrospective cohort study. BMC Musculoskeletal Disorders, 11(1), 155. https://doi.org/10.1186/1471-2474-11-155
Choi, E., Gil, H. Y., Ju, J., Han, W. K., Nahm, F. S., & Lee, P. B. (2022). Effect of nonsurgical spinal decompression on intensity of pain and herniated disc volume in subacute lumbar herniated disc. International Journal of Clinical Practice, 2022, 6343837. https://doi.org/10.1155/2022/6343837
Cosamalón-Gan, I., Cosamalón-Gan, T., Mattos-Piaggio, G., Villar-Suárez, V., García-Cosamalón, J., & Vega-Álvarez, J. A. (2021). Inflammation in the intervertebral disc herniation. Neurocirugía (English Edition), 32(1), 21-35. https://doi.org/10.1016/j.neucir.2020.01.001
Gherscovici, E. D., & Mayer, J. M. (2022). Relationship of healthy building determinants with back and neck pain: A systematic review. International Journal of Environmental Research and Public Health, 20(1), 815. https://doi.org/10.3390/ijerph20010815
Leemann, S., Peterson, C. K., Schmid, C., Anklin, B., & Humphreys, B. K. (2014). Outcomes of acute and chronic patients with magnetic resonance imaging-confirmed symptomatic lumbar disc herniations receiving high-velocity, low-amplitude, spinal manipulative therapy: A prospective observational cohort study with one-year follow-up. Journal of Manipulative and Physiological Therapeutics, 37(3), 155-163. https://doi.org/10.1016/j.jmpt.2014.01.002
PMC. (2008). Genetic and environmental influences on non-specific low back pain in children: A twin study. European Spine Journal, 17(4), 502-508. https://pmc.ncbi.nlm.nih.gov/articles/PMC2295279/
PMC. (2022). Relationship of healthy building determinants with back and neck pain: A systematic review. International Journal of Environmental Research and Public Health, 20(1), 815. https://pmc.ncbi.nlm.nih.gov/articles/PMC9755707/
Risk Factors Study. (2021). Risk factors of intervertebral disc pathology—A point of view formerly and today—A review. International Journal of Environmental Research and Public Health, 18(2), 726. https://pmc.ncbi.nlm.nih.gov/articles/PMC7865549/
Shokri, E., Kamali, F., Sinaei, E., & Ghafarinejad, F. (2018). Spinal manipulation in the treatment of patients with MRI-confirmed lumbar disc herniation and sacroiliac joint hypomobility: A quasi-experimental study. Chiropractic & Manual Therapies, 26, 16. https://doi.org/10.1186/s12998-018-0185-z
Turkish Journal of Medical Sciences. (2019). The incidence and most common levels of thoracic degenerative disc disease. Acta Orthopaedica et Traumatologica Turcica, 52(3), 195-200. https://pmc.ncbi.nlm.nih.gov/articles/PMC6657757/