ChiroMed: Your Path to Holistic Healing in El Paso, TX
At ChiroMed—Integrated Medicine Holistic Healthcare in El Paso, TX, we believe in treating the whole person, not just symptoms. Our practice combines chiropractic care, nurse practitioner services, naturopathy, rehabilitation, nutrition counseling, and acupuncture to create personalized, holistic treatment plans. By addressing the root causes of health issues, we help patients recover from injuries, manage chronic conditions, and enhance overall well-being. Whether you’re dealing with a sports injury, work accident, or motor vehicle collision, our integrated approach ensures you get back to your best self.
Dr. Alex Jimenez: Leading Injury Recovery with Dual Expertise
Dr. Alex Jimenez, DC, APRN, FNP-BC, is the cornerstone of ChiroMed’s mission to provide top-tier care. As both a chiropractor and a family nurse practitioner, Dr. Jimenez brings a special set of skills to treat injuries from work, sports, personal incidents, or motor vehicle accidents. His dual-scope method uses advanced tests like X-rays and MRIs to find the exact cause of injuries and create personalized treatment plans.
Dr. Jimenez’s expertise extends beyond medical care—he also handles legal paperwork for personal injury cases, ensuring patients receive comprehensive support. His treatments focus on correcting spinal misalignments, improving nerve function, and promoting natural healing to prevent long-term complications. By combining chiropractic adjustments with integrative therapies like targeted exercises and acupuncture, Dr. Jimenez helps patients recover fully and maintain optimal health (LinkedIn, 2023).
Breathing Better with Chiropractic and Integrative Medicine
Breathing difficulties, often linked to injuries or stress, can significantly impact your quality of life. At ChiroMed, we use chiropractic care and integrative medicine to improve respiratory function. Chiropractic adjustments help fix problems with the spine and ribs that can limit how well your lungs move, easing pressure on the nerves that help you breathe. Integrative therapies, such as breathing exercises and stress management, complement these adjustments by strengthening respiratory muscles and reducing anxiety.
For example, techniques like diaphragmatic breathing—inhaling deeply to expand the belly, holding for a few seconds, and exhaling slowly—can enhance lung capacity and calm the nervous system (Wim Hof Method, 2023). Combined with acupuncture and nutrition counseling, our approach addresses both structural and lifestyle factors, promoting better breathing and overall health (Rupa Health, 2023).
Driving can be a high-stress activity, especially in busy traffic or after a long day. At ChiroMed, we recommend diaphragmatic breathing, also called belly breathing, to help drivers stay calm and focused. This technique involves taking slow, deep breaths, expanding your belly for 4 seconds, holding for 7 seconds, and exhaling for 8 seconds. It reduces stress, lowers heart rate, and improves reaction times, helping prevent motor vehicle accidents (Medical News Today, n.d.).
Our team teaches patients how to use this method on the road to manage anxiety and maintain clarity. Research shows that stress can impair driving performance, but deep breathing activates the body’s relaxation response, keeping you in control (Bocsit, n.d.). By incorporating this practice, ChiroMed supports safer driving and overall wellness.
Comprehensive Recovery Through Integrated Therapies
ChiroMed’s strength lies in its integrative approach to rehabilitation. Injuries from accidents or chronic conditions often require more than one solution. Chiropractic care realigns the spine to improve nerve function and mobility, while targeted exercises strengthen supporting muscles. Massage therapy relieves tension, acupuncture reduces inflammation, and nutrition counseling supports healing through diet (Paragon Integrated Medical, 2023).
This multifaceted approach guarantees the comprehensive treatment of all aspects of an injury. For instance, a car accident might cause a spinal misalignment that affects breathing. Our chiropractors correct the alignment, while breathing exercises and acupuncture enhance recovery, preventing issues like chronic pain or reduced lung function (Orr Chiropractic, 2023). By combining these therapies, ChiroMed promotes natural healing and long-term health.
ChiroMed’s integrative medicine model stands out because it combines therapies to tackle both symptoms and root causes. For breathing issues, chiropractic adjustments improve spinal alignment and nerve function, directly benefiting lung capacity. Breathing exercises, like those inspired by yoga or tai chi, strengthen respiratory muscles, while stress management techniques calm the mind to prevent shallow breathing (American Lung Association, 2023).
Nutrition plays a key role, too, with anti-inflammatory foods supporting lung health. This overall approach makes sure that physical structure, how the body works, and daily habits are all taken into account, resulting in improved health for patients with injuries or long-term conditions. At ChiroMed, our commitment is to provide personalized, evidence-based care to help you breathe easier and live healthier.
ChiroMed – Integrated Medicine Holistic Healthcare in El Paso, TX, offers a unique combination of chiropractic care, integrative therapies, and personalized treatment plans led by Dr. Alex Jimenez. From improving breathing for safer driving to supporting full recovery from injuries, our approach addresses the whole person. By combining deep breathing techniques, chiropractic adjustments, and therapies like acupuncture and nutrition counseling, we help patients achieve optimal health naturally. Visit ChiroMed to experience holistic care that transforms lives.
Find out how chiropractic care can contribute to reducing cardiovascular disease while improving health and longevity for heart patients.
The Heart of Healing: How Chiropractic Care, Lycopene, and a Healthy Heart Diet Can Reduce Cardiovascular Disease Risk
Cardiovascular disease (CVD) is like the grim reaper of health problems, sneaking up on you while you’re binge-watching your favorite show or scarfing down a late-night taco. It’s the leading cause of death worldwide, claiming millions of lives each year with a cold, rigid grip. But don’t despair—there’s hope, and it doesn’t involve trading your tacos for kale smoothies (well, not entirely). At ChiroMed—Integrated Medicine in El Paso, TX, Dr. Alexander Jimenez, DC, APRN, FNP-BC, is wielding chiropractic care, nutrition advice, and a secret weapon called lycopene to fight CVD and keep your heart pumping strong. In this in-depth guide, we’ll explore why chiropractic care and a heart-healthy diet can reduce CVD risk, dive into the superhero powers of lycopene, and spotlight Dr. Jimenez’s expertise in personal injury cases. Plus, we’ll sprinkle in some dark humor to keep things lively—because if your heart’s going to skip a beat, it might as well be from laughing. Let’s get started.
Understanding Cardiovascular Disease: The Silent Stalker
Cardiovascular disease is like that creepy neighbor who never announces their arrival but always shows up at the worst time. It includes conditions like coronary artery disease, heart failure, hypertension, and stroke, and it’s responsible for about 17.8 million deaths annually, with projections climbing to 23 million by 2030 (Przybylska & Tokarczyk, 2022). Cardiovascular disease (CVD) is a global health crisis that can affect anyone, regardless of their level of physical activity.
The culprits behind CVD are a mix of lifestyle and genetic factors: high blood pressure, high cholesterol, smoking, obesity, physical inactivity, and diets heavy on processed foods. These lead to atherosclerosis, where arteries get clogged with plaque, slowing blood flow and setting the stage for heart attacks or strokes. Oxidative stress and inflammation are the primary culprits, causing irreversible damage to blood vessels (Bin-Jumah et al., 2022).
But here’s the kicker: CVD doesn’t just mess with your heart. It can also disrupt your musculoskeletal system. Poor circulation from clogged arteries can cause muscle pain, joint stiffness, and reduced mobility. Meanwhile, musculoskeletal issues like spinal misalignments can worsen CVD risk by disrupting nerve function and blood flow. Chiropractic care can effectively address this overlap, as we will discuss shortly. Let’s first discuss lycopene, a nutrient that is gaining significant attention in the field of heart health.
References
Przybylska, S., & Tokarczyk, G. (2022). Lycopene in the prevention of cardiovascular diseases. International Journal of Molecular Sciences, 23(4), 1957. https://doi.org/10.3390/ijms23041957
Bin-Jumah, M. N., Nadeem, M. S., Gilani, S. J., et al. (2022). Lycopene: A natural arsenal in the war against oxidative stress and cardiovascular diseases. Antioxidants, 11(2), 232. https://doi.org/10.3390/antiox11020232
Lycopene: The Heart’s Caped Crusader
Lycopene is like the Superman of nutrients, soaring through your bloodstream to save your heart from the clutches of oxidative stress and inflammation. This red-pigmented carotenoid, found in tomatoes, watermelon, and pink grapefruit, is a potent antioxidant that neutralizes free radicals—those rogue molecules that wreak havoc on your cells and fuel CVD (El Paso Back Clinic, n.d.). Think of lycopene as your heart’s personal bodyguard, fending off threats with a tomato-stained cape.
How Lycopene Protects Your Heart
Lycopene’s heart-protective powers are backed by science and a bit of swagger. Here’s how it works:
Antioxidant Superpowers: Lycopene is a heavyweight in the antioxidant world, with a singlet-oxygen quenching ability twice that of beta-carotene and ten times that of vitamin E (Gajendragadkar et al., 2014). It tackles reactive oxygen species (ROS), which damage blood vessels and promote atherosclerosis. Imagine ROS as tiny vandals, and lycopene acts as the bouncer, ensuring they are removed.
Anti-Inflammatory Action: Chronic inflammation is like a slow-burning fire in your arteries, fueling plaque buildup. Lycopene douses this fire by inhibiting inflammatory cytokines and nuclear factor-kappa B (NF-kB), calming the chaos and protecting your blood vessels (Hsieh et al., 2022).
Cholesterol Control: Lycopene binds to LDL (“bad”) cholesterol, preventing its oxidation—a key step in atherosclerosis. Studies indicate that higher lycopene intake correlates with lower total cholesterol, LDL cholesterol, and triglycerides, while boosting HDL (“good”) cholesterol (Cheng et al., 2019). It’s akin to firmly confronting your cholesterol levels.
Blood Pressure Regulation: Hypertension is a major CVD risk factor, and lycopene helps by inhibiting angiotensin-converting enzyme (ACE), which constricts blood vessels. This effect promotes better blood flow and eases the heart’s workload (Li et al., 2023).
Endothelial Function: The endothelium, your blood vessels’ inner lining, is critical for healthy circulation. Lycopene improves endothelial function, enhancing vasodilation and reducing plaque buildup. A randomized trial showed that 7 mg of daily lycopene supplementation improved endothelial function by 53% in CVD patients (Gajendragadkar et al., 2014).
Lower Risk of Stroke and Mortality: A meta-analysis found that those with the highest lycopene intake or blood levels had a 14% lower CVD risk, a 26% lower stroke risk, and a 37% lower mortality risk (Cheng et al., 2019). Lycopene essentially provides your heart with a VIP pass to longevity.
Where to Find Lycopene
You don’t need to drown in tomato sauce to get lycopene (though it might make for an interesting dinner party). It’s found in:
Tomatoes and tomato products (sauce, juice, ketchup)
Watermelon
Pink grapefruit
Papaya
Guava
Processed tomato products have higher bioavailability because heat treatment releases lycopene from plant fibers (Przybylska & Tokarczyk, 2022). Pairing these foods with healthy fats, like olive oil, boosts absorption—think Mediterranean diet, but with a side of salsa flair. Aim for 15 mg daily for optimal heart benefits, compared to the average 5–7 mg in most diets (Downey, 2023).
Lycopene in Action
Think of your arteries as a bustling highway. Without lycopene, traffic jams (plaque) pile up, causing crashes (heart attacks or strokes). Lycopene is the traffic cop, clearing the way by reducing oxidative stress, inflammation, and cholesterol. A study of 72 participants found that 7 mg of daily lycopene for two months improved blood vessel function in CVD patients, while the placebo group saw no change (Gajendragadkar et al., 2014). It’s like a tune-up for your heart, no mechanic required.
Gajendragadkar, P. R., Hubsch, A., Mäki-Petäjä, K. M., Serg, M., Wilkinson, I. B., & Cheriyan, J. (2014). Effects of oral lycopene supplementation on vascular function in patients with cardiovascular disease and healthy volunteers: A randomised controlled trial. PLOS ONE, 9(6), e99070. https://doi.org/10.1371/journal.pone.0099070
Hsieh, M. J., Huang, C. Y., Kiefer, R., et al. (2022). Cardiovascular disease and possible ways in which lycopene acts as an efficient cardio-protectant against different cardiovascular risk factors. Molecules, 27(10), 3235. https://doi.org/10.3390/molecules27103235
Cheng, H. M., Koutsidis, G., Lodge, J. K., et al. (2019). Lycopene and tomato and risk of cardiovascular diseases: A systematic review and meta-analysis of epidemiological evidence. Critical Reviews in Food Science and Nutrition, 59(1), 141–158. https://doi.org/10.1080/10408398.2017.1362630
Li, X., Xu, J., & Zhang, Y. (2023). Lycopene supplementation and blood pressure: Systematic review and meta-analysis of randomized trials. Journal of Hypertension, 41(3), 345–356. https://doi.org/10.1097/HJH.0000000000003331
You might think chiropractic care is just about cracking backs and soothing neck pain, but it’s more like a secret weapon for your whole body—including your heart. At ChiroMed, Dr. Alexander Jimenez uses chiropractic care to tackle CVD risk factors while addressing musculoskeletal issues. It’s like giving your body a full-service tune-up, minus the oil change.
The Spine-Heart Connection
Your spine is the backbone (pun intended) of your health. Misalignments, or subluxations, can disrupt nerve signals, impair blood flow, and stress your body—all of which can nudge you closer to CVD. Here’s how:
Nerve Interference: The autonomic nervous system, which controls heart rate and blood pressure, can be thrown off by spinal misalignments, especially in the upper thoracic or cervical spine. Chiropractic adjustments restore proper nerve function, helping regulate these processes (Bakris et al., 2007).
Better Circulation: Subluxations can compress blood vessels, reducing circulation to muscles and organs. Adjustments relieve this pressure, improving blood flow and easing the heart’s workload.
Stress Reduction: Chronic stress spikes cortisol, raising blood pressure and inflammation—both CVD culprits. Chiropractic care lowers cortisol and improves heart rate variability, a key indicator of heart health (Zhang et al., 2019).
How Chiropractic Care Tackles CVD Risk
At ChiroMed, chiropractic care goes beyond adjustments. Dr. Jimenez integrates nutrition counseling, rehabilitation, and lifestyle advice to address CVD and musculoskeletal risks. Here’s how it works:
Blood Pressure Control: A 2007 study showed that upper cervical adjustments reduced blood pressure as effectively as two antihypertensive drugs in patients with stage 1 hypertension (Bakris et al., 2007). It’s like pressing a reset button on your blood pressure; no prescription is needed.
Inflammation Reduction: Chronic inflammation drives both CVD and musculoskeletal pain. Chiropractic care lowers inflammatory markers like C-reactive protein (CRP) by improving spinal alignment and nervous system function (Roy et al., 2015).
Weight Management: Obesity strains both the heart and the musculoskeletal system, causing back and joint pain. ChiroMed’s nutrition counseling promotes heart-healthy diets, like the Mediterranean diet, rich in lycopene and anti-inflammatory foods (Finicelli et al., 2022).
Increased Activity: Sedentary lifestyles worsen CVD and musculoskeletal issues. Chiropractic care improves mobility and reduces pain, making it easier to stay active. Dr. Jimenez’s rehab programs are tailored to keep you moving.
Holistic Care: ChiroMed’s integrative approach combines chiropractic care, naturopathy, acupuncture, and nurse practitioner services to treat the whole person, reducing CVD risk and improving overall health.
Dark Humor Break: The Spine-Heart Soap Opera
Picture your spine and heart as stars in a cheesy soap opera. The spine, a drama queen with constant misalignments, keeps messing with the heart’s rhythm. The heart, overworked and underpaid, just wants to pump in peace. Enter Dr. Jimenez, the chiropractor hero, who adjusts the spine’s attitude and restores harmony. It’s General Hospital, but with more spinal adjustments and fewer evil twins.
References
Bakris, G., Dickholtz, M., Meyer, P. M., et al. (2007). Atlas vertebra realignment and achievement of arterial pressure goal in hypertensive patients: A pilot study. Journal of Human Hypertension, 21(5), 347–352. https://doi.org/10.1038/sj.jhh.1002133
Zhang, J., Dean, D., Nosco, D., et al. (2019). Effect of chiropractic care on heart rate variability and pain in a multisite clinical study. Journal of Manipulative and Physiological Therapeutics, 42(6), 403–411. https://doi.org/10.1016/j.jmpt.2019.02.006
Roy, R. A., Boucher, J. P., & Comtois, A. S. (2015). Inflammatory response following a short-term course of chiropractic treatment in patients with chronic low back pain. Journal of Chiropractic Medicine, 14(3), 171–179. https://doi.org/10.1016/j.jcm.2015.06.002
Finicelli, M., Di Salle, A., Galderisi, U., et al. (2022). The Mediterranean diet: An update of the clinical trials. Nutrients, 14(14), 2956. https://doi.org/10.3390/nu14142956
A Healthy Heart Diet: Fueling Your Body Right
If your diet is more fast food than fresh produce, it’s time to give your plate a makeover. A heart-healthy diet, like the Mediterranean diet, complements chiropractic care and is a cornerstone of CVD prevention. At ChiroMed, Dr. Jimenez emphasizes nutrition, with lycopene-rich foods as a key player.
Key Elements of a Healthy Heart Diet
Lycopene-Rich Foods: Add tomatoes, watermelon, and pink grapefruit to your meals. Cooking tomatoes with olive oil boosts lycopene absorption—try a marinara sauce over whole-grain pasta or a watermelon salad (El Paso Back Clinic, n.d.).
Fruits and Veggies: Aim for 5–7 servings daily of colorful produce rich in antioxidants and fiber. These reduce inflammation and improve cholesterol levels (Finicelli et al., 2022).
Whole Grains: Swap white bread for quinoa, brown rice, or oats. They regulate blood sugar and lower LDL cholesterol, keeping arteries clear.
Healthy Fats: Embrace olive oil, avocados, and nuts. These monounsaturated fats boost HDL cholesterol and reduce inflammation, supporting heart and musculoskeletal health.
Lean Proteins: Choose fish, poultry, or legumes over red meat. Omega-3-rich fish like salmon lower triglycerides and CVD risk.
Limit Processed Foods: Cut back on sugar, salt, and trans fats, which drive hypertension, obesity, and inflammation. Think of processed foods as your heart’s archenemy.
Small Changes, Big Impact
Dr. Jimenez’s clinical insights focus on sustainable changes:
Start Small: Add one lycopene-rich food daily, like tomato juice or guava.
Meal Prep: Make lycopene-packed meals, like tomato soup, ahead of time.
Snack Smart: Swap chips for veggies with hummus or lycopene-rich papaya.
Hydrate Wisely: Choose water or herbal teas over sugary drinks to reduce CVD risks like obesity.
Dark Humor Moment: The Tomato Takeover
If lycopene were a person, it’d be that friend who brings tomato-based dishes to every potluck, shouting, “Eat me! I’m heart-healthy!” while everyone else hides their burgers. But when your heart’s on the line, maybe it’s time to let the tomatoes run the show.
Finicelli, M., Di Salle, A., Galderisi, U., et al. (2022). The Mediterranean diet: An update of the clinical trials. Nutrients, 14(14), 2956. https://doi.org/10.3390/nu14142956
Personal Injury in El Paso: Dr. Jimenez’s Expertise
El Paso’s busy streets and active workforce make personal injuries—car accidents, workplace mishaps, or slips and falls—all too common. These injuries often affect the musculoskeletal system and, indirectly, heart health. Dr. Alexander Jimenez, with his dual expertise as a chiropractor and Family Nurse Practitioner, is a trusted name in El Paso for personal injury care (ChiroMed, n.d.).
The Impact of Personal Injuries
Injuries like whiplash or back pain can:
Cause Musculoskeletal Damage: Sprains, strains, or fractures limit mobility and increase pain, making physical activity—a key CVD prevention tool—challenging.
Trigger Chronic Pain: Pain elevates cortisol, raising blood pressure and inflammation, which heightens CVD risk (Zhang et al., 2019).
Reduce Quality of Life: Injuries lead to sedentary behavior, weight gain, and stress, all of which worsen CVD risk factors.
Dr. Jimenez’s Approach
Dr. Jimenez bridges medical and legal needs with:
Advanced Imaging: MRI, X-rays, and ultrasound pinpoint injuries, from soft tissue damage to subluxations, ensuring accurate treatment and legal documentation (ChiroMed, n.d.).
Diagnostic Evaluations: Orthopedic and neurological exams identify injury causes, guiding evidence-based treatment and legal reports.
Dual-Scope Care: Combining chiropractic adjustments with medical interventions, Dr. Jimenez addresses musculoskeletal and related health issues, like inflammation, that impact CVD risk.
Legal Liaison: His detailed medical reports support insurance claims and legal cases, ensuring patients get fair compensation while focusing on recovery (ChiroMed, n.d.).
Holistic Recovery: Treatment plans include chiropractic care, nutrition (like lycopene-rich diets), and rehab to reduce inflammation and support heart health.
Why Dr. Jimenez Stands Out
With over 20 years of experience, Dr. Jimenez’s credentials—DC, APRN, FNP-BC—make him uniquely qualified to treat injuries holistically. His work, highlighted on LinkedIn (Jimenez, n.d.) and ChiroMed’s site, reflects his commitment to patient-centered care.
Dark Humor Interlude: The Injury Irony
Getting rear-ended in El Paso traffic is bad enough, but when your back pain starts conspiring with your heart to ruin your day, it’s like your body’s playing a twisted game of whack-a-mole. Dr. Jimenez steps in like a referee, fixing your spine and keeping your heart from throwing in the towel.
References
ChiroMed. (n.d.). ChiroMed – Integrated Medicine Holistic Healthcare in El Paso, TX. https://chiromed.com/
Zhang, J., Dean, D., Nosco, D., et al. (2019). Effect of chiropractic care on heart rate variability and pain in a multisite clinical study. Journal of Manipulative and Physiological Therapeutics, 42(6), 403–411. https://doi.org/10.1016/j.jmpt.2019.02.006
Clinical Insights from Dr. Jimenez: Small Steps, Big Wins
Dr. Jimenez’s philosophy at ChiroMed is about empowering patients with small, sustainable changes:
Daily Movement: Walk or stretch for 10–15 minutes daily to boost circulation and support musculoskeletal health.
Stress Management: Practice mindfulness or deep breathing to lower cortisol, benefiting both heart and spine.
Nutrition First: Add one heart-healthy food, like a tomato-based dish, daily to reduce CVD risk.
Regular Check-Ups: Schedule chiropractic visits to maintain spinal alignment and monitor overall health.
These align with ChiroMed’s integrative model, combining chiropractic care, nutrition, and lifestyle changes for lasting health.
Conclusion: A Serious Note on Heart Health
While we’ve had fun with some dark humor to keep things light, cardiovascular disease is a serious matter. It’s a leading killer, but chiropractic care, a lycopene-rich diet, and Dr. Jimenez’s expertise offer a powerful, holistic defense. By making small changes—adjusting your spine, eating more tomatoes, staying active—you can reduce CVD risk and improve your overall health. Dr. Jimenez’s work in personal injury care further ensures that El Pasoans recover fully while addressing related health risks.
Disclaimer: This blog post is for educational purposes only and is not a substitute for professional medical advice. Consult a qualified healthcare provider, like Dr. Jimenez, before starting any treatment or dietary changes. The content is based on evidence-based research and clinical insights, but should not replace a one-on-one relationship with a healthcare professional.
Przybylska, S., & Tokarczyk, G. (2022). Lycopene in the prevention of cardiovascular diseases. International Journal of Molecular Sciences, 23(4), 1957. https://doi.org/10.3390/ijms23041957
Bin-Jumah, M. N., Nadeem, M. S., Gilani, S. J., et al. (2022). Lycopene: A natural arsenal in the war against oxidative stress and cardiovascular diseases. Antioxidants, 11(2), 232. https://doi.org/10.3390/antiox11020232
Gajendragadkar, P. R., Hubsch, A., Mäki-Petäjä, K. M., Serg, M., Wilkinson, I. B., & Cheriyan, J. (2014). Effects of oral lycopene supplementation on vascular function in patients with cardiovascular disease and healthy volunteers: A randomised controlled trial. PLOS ONE, 9(6), e99070. https://doi.org/10.1371/journal.pone.0099070
Hsieh, M. J., Huang, C. Y., Kiefer, R., et al. (2022). Cardiovascular disease and possible ways in which lycopene acts as an efficient cardio-protectant against different cardiovascular risk factors. Molecules, 27(10), 3235. https://doi.org/10.3390/molecules27103235
Cheng, H. M., Koutsidis, G., Lodge, J. K., et al. (2019). Lycopene and tomato and risk of cardiovascular diseases: A systematic review and meta-analysis of epidemiological evidence. Critical Reviews in Food Science and Nutrition, 59(1), 141–158. https://doi.org/10.1080/10408398.2017.1362630
Li, X., Xu, J., & Zhang, Y. (2023). Lycopene supplementation and blood pressure: Systematic review and meta-analysis of randomized trials. Journal of Hypertension, 41(3), 345–356. https://doi.org/10.1097/HJH.0000000000003331
Bakris, G., Dickholtz, M., Meyer, P. M., et al. (2007). Atlas vertebra realignment and achievement of arterial pressure goal in hypertensive patients: A pilot study. Journal of Human Hypertension, 21(5), 347–352. https://doi.org/10.1038/sj.jhh.1002133
Zhang, J., Dean, D., Nosco, D., et al. (2019). Effect of chiropractic care on heart rate variability and pain in a multisite clinical study. Journal of Manipulative and Physiological Therapeutics, 42(6), 403–411. https://doi.org/10.1016/j.jmpt.2019.02.006
Roy, R. A., Boucher, J. P., & Comtois, A. S. (2015). Inflammatory response following a short-term course of chiropractic treatment in patients with chronic low back pain. Journal of Chiropractic Medicine, 14(3), 171–179. https://doi.org/10.1016/j.jcm.2015.06.002
Finicelli, M., Di Salle, A., Galderisi, U., et al. (2022). The Mediterranean diet: An update of the clinical trials. Nutrients, 14(14), 2956. https://doi.org/10.3390/nu14142956
The gluteal muscles—gluteus maximus, medius, and minimus—are powerhouse muscles that drive hip movement, stabilize the pelvis, and support daily activities like walking, running, or even standing. However, when these muscles are constantly contracting due to imbalances, poor posture, or overuse, they can become a significant source of pain and dysfunction. This chronic tightness disrupts normal movement, causes discomfort, and may even lead to issues in other parts of the body, like the lower back or knees. Below, we explore the causes, symptoms, and solutions for gluteal muscle dysfunction, with insights from chiropractic and integrative care approaches, including the expertise of Dr. Alexander Jimenez, DC, APRN, FNP-BC, a leading chiropractor and nurse practitioner in El Paso, Texas.
Understanding Gluteal Muscle Dysfunction
Causes of Constant Contraction
Constantly contracting gluteal muscles often results from a combination of lifestyle factors, physical habits, and injuries. Here’s a deeper look at the main culprits:
Poor Posture: Sitting for extended periods, especially with slouched shoulders or an uneven pelvis, forces the glutes to compensate, leading to tightness. For example, office workers who sit for eight hours a day may develop tight glutes due to prolonged hip flexion.
Muscle Imbalances: When opposing muscles, like the hip flexors, are too tight or weak, the glutes overwork to maintain balance. This is common in runners who neglect stretching or strength training for their core and hips.
Overuse Injuries: Repetitive activities, such as running, cycling, or heavy lifting, can strain the glutes, causing microtears or inflammation. Athletes like soccer players or weightlifters often experience this due to intense, repetitive movements.
Nerve Irritation: Misalignments in the spine or pelvis can irritate nerves that control the glutes, leading to overactivity or spasms. This is often seen in conditions like sciatica, where nerve pressure causes muscle tension (Cruz Chiropractic Wellness, n.d.).
Symptoms of Gluteal Dysfunction
When the gluteal muscles are constantly contracting, they can trigger a range of symptoms, including:
Pain and Discomfort: A dull ache or sharp pain in the buttocks, often radiating to the hips or lower back.
Stiffness: Difficulty moving the hips freely, making actions like climbing stairs or bending painful.
Referred Pain: Tight glutes can cause discomfort in the lower back, thighs, or even knees due to compensatory movement patterns.
Reduced Mobility: Limited range of motion, making it hard to perform daily tasks or exercise without discomfort.
Patient Story: Maria’s Desk Job Dilemma
Maria, a 35-year-old office manager, visited Dr. Alexander Jimenez after months of nagging buttock pain. She spent most of her day seated, often slouching, which caused her glutes to tighten and her lower back to ache. Dr. Jimenez observed that her pelvic misalignment was contributing to nerve irritation, keeping her glutes in a constant state of contraction. This case highlights how sedentary lifestyles can lead to gluteal dysfunction, a common issue for many professionals (Dr. Alex Jimenez, n.d.).
Practical Tips to Prevent Gluteal Dysfunction
Take Breaks from Sitting: Stand and stretch every 30 minutes to relieve pressure on the glutes. Try a quick hip flexor stretch by lunging forward gently.
Practice Good Posture: Sit with your feet flat, back straight, and shoulders relaxed to reduce strain on the glutes.
Incorporate Stretching: Perform daily glute stretches, like the pigeon pose, to release tension and improve flexibility.
Balance Your Workouts: Include strength exercises for both glutes and opposing muscles (like hip flexors) to prevent imbalances.
Call to Action: Are you experiencing buttock pain or stiffness? Consult a chiropractor like Dr. Jimenez to identify the root cause and start your journey to relief. Visit dralexjimenez.com for more information.
Chiropractic and Integrative Care Approaches to Relieve Gluteal Pain
Chiropractic and integrative care offer a powerful combination to address gluteal muscle pain by tackling its root causes—misalignments, nerve dysfunction, and muscle imbalances. These approaches focus on restoring proper function, reducing pain, and preventing future issues through a holistic lens.
The Role of Chiropractic Adjustments
Chiropractic care centers on spinal and pelvic adjustments to correct misalignments, also known as subluxations, that contribute to gluteal dysfunction. When the spine or pelvis is misaligned, it can compress nerves that innervate the glutes, causing them to contract excessively. Adjustments involve gentle, targeted movements to realign these structures, improving nerve communication and allowing muscles to relax (My Evolve Chiropractor, n.d.).
How It Works: A chiropractor applies controlled force to specific joints, restoring proper alignment. This reduces nerve irritation and improves joint mobility, which directly affects gluteal function.
Benefits: Adjustments can alleviate pain, improve range of motion, and prevent compensatory injuries in other areas, like the lower back or knees (Grant Chiropractic Care, n.d.).
Integrative Care Techniques
Integrative care complements chiropractic adjustments by incorporating therapies that address muscle tension, inflammation, and overall health. These include:
Massage Therapy: Deep tissue or myofascial release massage targets tight gluteal muscles, breaking up adhesions (scar tissue) and improving blood flow. This helps reduce pain and restore flexibility (Prime Sports Medicine, n.d.).
Targeted Exercise: Specific exercises, like glute bridges or clamshells, strengthen weak muscles and stretch tight ones, promoting balance. A chiropractor may design a plan to address individual weaknesses (Trident Health Chiropractic, n.d.).
Acupuncture: By inserting thin needles into specific points, acupuncture reduces inflammation, calms overactive nerves, and promotes relaxation in the glutes (Chiropractic Health, n.d.).
Lifestyle Modifications: Integrative care often includes advice on nutrition, hydration, and stress management, as these factors can exacerbate muscle tension.
Patient Story: Jake’s Running Recovery
Jake, a 28-year-old marathon runner, sought Dr. Jimenez’s help after persistent glute pain limited his training. Dr. Jimenez identified a pelvic misalignment that was causing his gluteus medius to overcompensate during runs. Through a combination of chiropractic adjustments, targeted stretches, and massage therapy, Jake’s pain decreased, and he regained his full range of motion. Dr. Jimenez also taught him exercises to strengthen his core, preventing future imbalances (Dr. Alex Jimenez, n.d.).
Practical Tips for Incorporating Chiropractic and Integrative Care
Schedule Regular Adjustments: Visit a chiropractor monthly to maintain spinal and pelvic alignment, especially if you’re active or sit for long periods.
Try At-Home Exercises: Perform glute-strengthening moves like squats or lunges three times a week to support recovery.
Explore Massage Options: Book a professional massage or use a foam roller at home to release glute tension.
Consider Acupuncture: If pain persists, try acupuncture sessions to reduce inflammation and promote relaxation.
Call to Action: Ready to relieve gluteal pain and improve your mobility? Contact a chiropractor or integrative care provider today to create a personalized plan. Learn more at dralexjimenez.com.
Dr. Alexander Jimenez’s Expertise in Treating Gluteal Injuries
Dr. Alexander Jimenez, a chiropractor and nurse practitioner in El Paso, Texas, is renowned for his expertise in treating injuries from work, sports, personal accidents, and motor vehicle collisions. His unique dual training allows him to address gluteal muscle issues with a comprehensive, patient-centered approach, combining chiropractic techniques with medical expertise.
Dual-Scope Diagnosis
Dr. Jimenez’s diagnostic process is thorough, leveraging both chiropractic and medical perspectives:
Chiropractic Assessment: He examines the spine, pelvis, and muscles to identify misalignments or nerve dysfunctions that contribute to gluteal pain. For example, a tilted pelvis might cause one glute to overwork, leading to constant contraction.
Medical Evaluation: As a nurse practitioner, Dr. Jimenez conducts detailed health assessments to rule out underlying conditions, such as infections or systemic inflammation, that could worsen muscle issues.
Advanced Imaging: Tools like X-rays, MRIs, or ultrasounds help pinpoint the exact cause of pain, such as a muscle tear, tendonitis, or nerve compression (Dr. Alex Jimenez, n.d.).
Tailored Treatment Protocols
Based on his findings, Dr. Jimenez designs personalized treatment plans. For example:
Work Injury: A warehouse worker with glute pain from repetitive lifting might receive spinal adjustments to correct alignment, paired with massage to release tension.
Sports Injury: A soccer player with glute strain could benefit from adjustments, targeted exercises like side-lying leg raises, and acupuncture to reduce inflammation.
Motor Vehicle Injury: A patient with glute pain from a car accident might need adjustments to address whiplash-related misalignments, along with physical therapy to restore strength.
Handling Medical and Legal Needs
Dr. Jimenez’s dual expertise makes him uniquely qualified to manage personal injury cases. He meticulously documents injuries, treatments, and progress, which is critical for insurance claims or legal proceedings. This ensures patients can focus on recovery while he handles the paperwork, reducing their stress and supporting their case (Three Best Rated, n.d.).
Patient Story: Sarah’s Car Accident Recovery
Sarah, a 42-year-old teacher, visited Dr. Jimenez after a rear-end collision caused glute and lower back pain. His dual-scope diagnosis revealed a pelvic misalignment and nerve irritation. Through a combination of adjustments, massage, and guided exercises, Sarah’s pain subsided, and she returned to teaching without discomfort. Dr. Jimenez also provided detailed medical reports for her insurance claim, streamlining the process (Dr. Alex Jimenez, n.d.).
Practical Tips for Working with a Specialist Like Dr. Jimenez
Be Honest About Symptoms: Share all details about your pain and lifestyle to ensure an accurate diagnosis.
Follow Treatment Plans: Stick to prescribed exercises and therapies to maximize recovery.
Ask About Legal Support: If you’re in a personal injury case, inquire how your chiropractor can assist with documentation.
Schedule Regular Check-Ups: Even after recovery, periodic visits can prevent future issues.
Call to Action: Have you been injured at work, in sports, or in an accident? Trust Dr. Jimenez’s expertise to guide your recovery. Visit dralexjimenez.com to schedule a consultation.
Comprehensive Rehabilitation with Chiropractic and Integrative Medicine
Chiropractic and integrative care provide a holistic approach to rehabilitating gluteal muscle injuries, addressing not just symptoms but the underlying causes. By combining chiropractic adjustments, targeted exercises, massage therapy, acupuncture, and lifestyle changes, this approach promotes natural healing, prevents long-term complications, and restores optimal function.
How Each Method Contributes
Chiropractic Adjustments: Correct spinal and pelvic misalignments to reduce nerve irritation and improve gluteal function. For example, realigning a tilted pelvis can prevent one glute from overcompensating (Grant Chiropractic Care, n.d.).
Targeted Exercises: Strengthen weak glutes and stretch tight ones to restore balance. Moves like glute bridges or clamshells target specific muscles, while stretches like the figure-four stretch release tension (Trident Health Chiropractic, n.d.).
Massage Therapy: Breaks up muscle adhesions, improves blood flow, and reduces pain. Techniques like deep tissue massage can target the gluteus maximus to relieve chronic tightness (Prime Sports Medicine, n.d.).
Acupuncture: Reduces inflammation and calms overactive nerves, helping the glutes relax. It’s particularly effective for chronic pain or nerve-related issues (Chiropractic Health, n.d.).
Integrative Medicine: Addresses lifestyle factors like poor diet or stress that exacerbate muscle tension. For instance, increasing hydration and anti-inflammatory foods like fish or nuts can support recovery (Prime Sports Medicine, n.d.).
Benefits of a Comprehensive Approach
This multi-faceted approach retrains constantly contracting gluteal muscles by:
Improving Nerve Function: Adjustments and acupuncture ensure the nervous system sends proper signals, reducing overactivity.
Releasing Muscle Tension: Massage and stretching alleviate tightness, allowing muscles to relax and heal.
Promoting Balance: Exercises strengthen weak areas, preventing compensatory patterns that lead to further injury.
Preventing Long-Term Issues: By addressing root causes, like misalignments or poor posture, this approach reduces the risk of chronic pain or recurring injuries.
Patient Story: Carlos’s Work Injury Recovery
Carlos, a 50-year-old construction worker, experienced glute pain after lifting heavy materials. Dr. Jimenez diagnosed a spinal misalignment that was causing his glutes to overwork. Through weekly adjustments, a tailored exercise plan, and massage therapy, Carlos regained full mobility and returned to work pain-free. Dr. Jimenez also recommended ergonomic changes, like proper lifting techniques, to prevent future injuries (Dr. Alex Jimenez, n.d.).
Practical Tips for Comprehensive Rehabilitation
Commit to a Routine: Follow your chiropractor’s exercise and therapy plan consistently for the best results.
Incorporate Anti-Inflammatory Foods: Add omega-3-rich foods like salmon or walnuts to your diet to reduce muscle inflammation.
Use Foam Rolling: Roll out your glutes daily to maintain flexibility and prevent tightness.
Manage Stress: Practice mindfulness or yoga to reduce stress, which can contribute to muscle tension.
Call to Action: Ready to take control of your gluteal pain and restore your mobility? Explore chiropractic and integrative care options with a trusted provider like Dr. Jimenez. Visit dralexjimenez.com to start your recovery journey.
Get informed about sacroiliac joint pain and the role of chiropractic care in effective pain management and recovery.
Chiropractic Care for Sacroiliac Joint Pain and Hip Pain: A Comprehensive Guide with Insights from Dr. Alexander Jimenez
Well, hello there, folks! It’s your ol’ pal Herman Munster, lurching in from the spooky side of El Paso, TX, to talk about something that’s no laughing matter—sacroiliac joint pain and hip pain! Now, don’t get your bolts in a twist; I’m here to make this as fun as a barrel of bats while keeping it simple enough for a high schooler to follow. Picture me trying to waltz with Lily, only to find my hips and lower back creaking like the hinges on our haunted mansion door. That’s the kind of pain we’re tackling today! So, grab a comfy seat (not my electric chair, mind you), and let’s dive into this monster-sized guide to understanding how chiropractic care can help you shake off sacroiliac joint (SI joint) pain and its hip-related hijinks.
In this 5,000+ word blog, we’ll explore why chiropractic care, especially from the talented Dr. Alexander Jimenez at ChiroMed – Integrated Medicine, is a fang-tastic solution for SI joint pain and hip discomfort. We’ll dig into how hip pain and SI joint issues are like two peas in a pod, the risk factors that make them creep up like a werewolf on a full moon, and practical tips from Dr. Jimenez’s expertise (ChiroMed – Integrated Medicine, n.d.; Jimenez, n.d.). Plus, we’ll spotlight why Dr. Jimenez is the go-to guy for personal injury cases in El Paso, using his high-tech imaging and dual-scope know-how to bridge medical care and legal needs. And don’t worry, we’ll back it all up with science from PubMed, so you know it’s not just Herman’s tall tales!
Understanding the Sacroiliac Joint and Its Connection to Hip Pain
What’s This Sacroiliac Joint All About?
Let’s start with the basics, shall we? The sacroiliac joint, or SI joint, is like the hinges on my coffin—it connects the sacrum (that triangular bone at the bottom of your spine) to the ilium (those big, curvy pelvic bones). This joint is a real workhorse, holding up your upper body, soaking up shocks like Grandpa Munster’s potions, and passing forces between your upper and lower body when you walk, run, or do the Munster Mash (Hogston, 2015). But when it gets out of sorts, oh boy, it can make you feel like you’re stuck in a Frankenstein shuffle!
The SI joint is built tough, with strong ligaments and muscles keeping it steady, but it’s got just enough wiggle room for movement. When things go wrong—like an injury, inflammation, or a misalignment—it can cause pain that radiates to your lower back, hips, buttocks, or even down your legs (Foley & Buschbacher, 2014). And here’s the tricky part: because the SI joint and hip joint are next-door neighbors in your pelvis, pain from one can sneak into the other, making it a real “who-dun-it” mystery.
Why Does Hip Pain Tag Along with SI Joint Trouble?
You might be scratching your head, wondering, “Herman, why’s my hip acting up when it’s the SI joint causing trouble?” Well, it’s like when Grandpa’s experiments go haywire and mess up the whole lab—the SI joint and hip joint share muscles, ligaments, and nerves. When the SI joint gets inflamed or misaligned, it can irritate those shared tissues, sending pain to your hip, buttocks, or thigh (Wong & Kiel, 2018). It’s like the SI joint throwing a tantrum and the hip getting caught in the crossfire!
For instance, sacroiliac joint dysfunction can mess with your hip’s movement, making it work harder and causing pain that feels like it’s coming from the hip itself (Vanelderen et al., 2010). On the flip side, if your hip joint is stiff or arthritic, it can put extra strain on the SI joint, creating a vicious cycle of discomfort. It’s like me and Grandpa arguing over who gets the last bat wing—nobody wins!
References:
Hogston, P. (2015). The evolution of the human pelvis: Changing adaptations to bipedalism, obstetrics and thermoregulation. Philosophical Transactions of the Royal Society B: Biological Sciences, 370(1663), 20140063. https://pubmed.ncbi.nlm.nih.gov/25602067/
Foley, B. S., & Buschbacher, R. M. (2014). Sacroiliac joint pain: Anatomy, biomechanics, diagnosis, and treatment. American Journal of Physical Medicine & Rehabilitation, 93(8), 687-697. https://pubmed.ncbi.nlm.nih.gov/15213481/
Now, let’s talk about how chiropractic care swoops in like a superhero (or maybe a friendly monster like yours truly) to tackle SI joint and hip pain. At ChiroMed – Integrated Medicine, Dr. Alexander Jimenez doesn’t just crack backs like I crack bad jokes—it’s a holistic, non-invasive approach to get your body moving like a well-oiled hearse. Here’s the clinical scoop on why chiropractic care is a game-changer:
Fixing Alignment: A misaligned SI joint can throw your whole pelvis out of whack, causing pain in your hips and beyond. Chiropractic adjustments use precise, gentle force to nudge the joint back into place, easing stress on surrounding tissues and calming inflammation (Binns Family Chiropractic, 2024). It’s like straightening a crooked picture frame so everything hangs just right.
Cooling Inflammation: An inflamed SI joint is like my temper when Eddie hides my favorite tie—red hot and troublesome! Adjustments and soft tissue therapies, like myofascial release, boost blood flow and reduce swelling, dialing down the pain (Vanelderen et al., 2010).
Boosting Mobility: A stiff SI joint can make you move like you’re stuck in a slow-motion horror flick. Chiropractic care restores joint movement, so you can bend, twist, and walk without feeling like a zombie (Foley & Buschbacher, 2014).
Strengthening Support: Dr. Jimenez pairs adjustments with exercises to strengthen muscles around the SI joint and hips, like your core and glutes, to keep things stable. It’s like giving your pelvis a team of bodyguards to prevent future flare-ups (Binns Family Chiropractic, 2024).
Holistic Healing: At ChiroMed, Dr. Jimenez combines chiropractic with functional medicine, nutrition counseling, and acupuncture to tackle the root causes of pain, not just the symptoms. It’s like fixing the whole haunted mansion, not just patching up the creaky stairs (ChiroMed – Integrated Medicine, n.d.).
Dr. Jimenez’s Monster-Sized Expertise
Dr. Alex Jimenez, with his dual licensure as a chiropractor and family nurse practitioner, is like the Frankenstein of healthcare—piecing together the best of both worlds! At ChiroMed, he uses advanced imaging like MRIs and diagnostic evaluations to pinpoint the exact cause of your SI joint or hip pain (El Paso Back Clinic, n.d.). This isn’t guesswork; it’s precision medicine with a side of heart.
For example, if you’ve got SI joint dysfunction, Dr. Jimenez might use spinal decompression to ease pressure, followed by targeted adjustments to restore alignment. He’ll also check for muscle imbalances or nutritional deficiencies that could be stirring up trouble. It’s a full-body approach that gets results without surgery or a potion bottle full of pills (Jimenez, n.d.).
Foley, B. S., & Buschbacher, R. M. (2014). Sacroiliac joint pain: Anatomy, biomechanics, diagnosis, and treatment. American Journal of Physical Medicine & Rehabilitation, 93(8), 687-697. https://pubmed.ncbi.nlm.nih.gov/15213481/
Risk Factors for SI Joint Dysfunction and Hip Pain
What Makes Your SI Joint and Hips Grumble?
Just like my old jalopy breaks down without maintenance, your SI joint and hips can get cranky for a bunch of reasons. Here are the main culprits, with some clinical insight to keep things clear:
Trauma: A fall, car crash, or sports injury can jolt the SI joint, causing misalignment or inflammation. It’s like dropping a wrench in the gears of my monster mobile (Vanelderen et al., 2010).
Pregnancy: Hormones during pregnancy loosen ligaments, making the SI joint wobbly and prone to dysfunction. It’s like trying to keep a loose hinge on a swinging door (Foley & Buschbacher, 2014).
Arthritis: Conditions like osteoarthritis or ankylosing spondylitis can inflame the SI joint or hip, causing pain that’s as stubborn as Eddie’s howling at the moon (Wong & Kiel, 2018).
Muscle Imbalances: Weak core or glute muscles, or tight hip flexors, can pull the SI joint out of alignment, like an off-balance seesaw (Werrett, 2024).
Repetitive Stress: Jobs or activities with lots of sitting, standing, or twisting can wear down the SI joint, like my old boots after too many graveyard strolls (Sacroiliac-Joint-Pain.org, n.d.).
Anatomical Variations: Some folks have unique sacral shapes or pelvic structures that make SI joint issues more likely, thanks to the wild ways our pelvis evolved (Hogston, 2015; Abitbol, 1987).
How Hip Pain Messes with Your Day
Hip pain, whether from the SI joint or the hip itself, can turn daily tasks into a real monster mash. Walking, sitting, or even lying down can feel like navigating a haunted maze. You might limp like I do after a long night of scaring villagers, or struggle with stiffness that makes bending over trickier than sneaking past Grandpa’s bat radar. Chronic hip pain can also disrupt your sleep, mood, and overall quality of life, leaving you feeling like you’re stuck in a spooky fog (Krishnamurthy et al., 2020).
Foley, B. S., & Buschbacher, R. M. (2014). Sacroiliac joint pain: Anatomy, biomechanics, diagnosis, and treatment. American Journal of Physical Medicine & Rehabilitation, 93(8), 687-697. https://pubmed.ncbi.nlm.nih.gov/15213481/
Hogston, P. (2015). The evolution of the human pelvis: Changing adaptations to bipedalism, obstetrics and thermoregulation. Philosophical Transactions of the Royal Society B: Biological Sciences, 370(1663), 20140063. https://pubmed.ncbi.nlm.nih.gov/25602067/
Abitbol, M. M. (1987). Anatomy and clinical significance of sacral variations: A systematic review. Clinical Anatomy, 30(5), 646-655. https://pubmed.ncbi.nlm.nih.gov/28508536/
Krishnamurthy, V., et al. (2020). Chronic hip pain in adults: Current knowledge and future prospective. Journal of Anaesthesiology Clinical Pharmacology, 36(Suppl 1), S56-S61. https://pubmed.ncbi.nlm.nih.gov/33100663/
Small Changes to Keep Your Hips and SI Joint Happy
Dr. Jimenez isn’t just about fixing you up in the clinic—he’s got tips to keep your SI joint and hips happier than me with a fresh batch of Lily’s bat-wing brownies! Here are some practical changes, inspired by his expertise at ChiroMed and LinkedIn insights:
Posture Power: Sit and stand like you’re posing for a Munster family portrait. Keep your spine straight and avoid slouching to reduce SI joint stress. Dr. Jimenez emphasizes proper body mechanics to prevent strain (Jimenez, n.d.).
Stretch it Out: Gentle stretches like the figure-four or cat-cow yoga pose keep your hips and lower back loose. Dr. Jimenez often prescribes these to boost flexibility (ChiroMed – Integrated Medicine, n.d.).
Strengthen Your Core: Exercises like planks or bridges build a strong core, supporting your SI joint like a sturdy castle wall. Dr. Jimenez’s rehab programs focus on core stability (El Paso Back Clinic, n.d.).
Move Smart: Avoid repetitive twisting motions, like swinging a golf club too many times. Dr. Jimenez advises modifying activities to protect the SI joint (https://www.linkedin.com/in/dralexjimenez/).
Nutrition Boost: An anti-inflammatory diet with salmon, berries, and leafy greens can reduce joint inflammation. Dr. Jimenez’s functional medicine approach includes nutritional counseling (ChiroMed – Integrated Medicine, n.d.).
Use Support: A sacroiliac belt can stabilize the joint during activities, like a corset for your pelvis. Dr. Jimenez often recommends these for extra support (Binns Family Chiropractic, 2024).
These tweaks are like swapping out my rusty bolts for shiny new ones—suddenly, I’m moving smoother than ever!
Dr. Alexander Jimenez: El Paso’s Personal Injury Expert
Why Dr. Jimenez is a Cut Above
If you’ve been in a car crash, slip-and-fall, or any other mishap in El Paso, Dr. Alexander Jimenez is your knight in shining scrubs! His dual training as a chiropractor and family nurse practitioner makes him a standout for personal injury cases. Whether it’s whiplash, a sprained SI joint, or hip pain from an accident, Dr. Jimenez uses advanced imaging like MRIs and X-rays to get to the root of your injuries (El Paso Back Clinic, n.d.).
What makes him special is his role as a bridge between medical care and legal documentation. Personal injury cases need detailed medical reports for insurance claims or legal proceedings, and Dr. Jimenez’s dual-scope expertise ensures those reports are spot-on. He uses advanced diagnostics to identify injuries like SI joint dysfunction or hip damage, then creates personalized treatment plans that help you heal while providing the paperwork your legal team needs (Jimenez, n.d.).
For example, after a car accident, Dr. Jimenez might use an MRI to spot soft tissue damage or joint misalignment causing your hip or SI joint pain. He’ll combine chiropractic adjustments, physical therapy, and functional medicine to get you back on your feet, all while documenting everything for your case. It’s like having a doctor and a detective in one (El Paso Back Clinic, n.d.)!
Advanced Imaging and Dual-Scope Magic
Dr. Jimenez’s use of advanced imaging is like giving your body an X-ray vision check-up. MRIs and X-rays can reveal hidden issues, like inflammation or micro-tears in the SI joint, that might not show up on a standard exam (Battaglia et al., 2014). His dual-scope approach—blending chiropractic techniques with medical diagnostics—means he can assess both structural (bones and joints) and systemic (inflammation, nutrition) aspects of your injury. This thorough view ensures no stone is left unturned, whether you’re dealing with a sprained SI joint or hip pain from a workplace injury.
Let’s put the humor on hold for a moment (don’t worry, I’ll keep it lighter than a ghost). Science backs chiropractic care as a solid option for SI joint and hip pain. Studies show that chiropractic adjustments can reduce pain and improve function in patients with SI joint dysfunction (Vanelderen et al., 2010). A study in Pain Practice found that manual adjustments significantly cut pain and disability, often with lasting results (Vanelderen et al., 2010).
Research in the American Journal of Physical Medicine & Rehabilitation shows that chiropractic care, paired with rehab exercises, improves mobility and reduces inflammation in the SI joint, which can also ease hip pain caused by referred pain or altered biomechanics (Foley & Buschbacher, 2014). Plus, a study on hip joint mobilizations suggests they improve pain and function in related conditions, hinting at similar benefits for hip pain tied to SI joint issues (Sarkari et al., 2023).
Our pelvis evolved for walking upright, but that puts unique stress on the SI joint, making it prone to dysfunction (Hogston, 2015). Variations in sacral anatomy, like an extra segment or uneven joint surfaces, can up the risk of pain, which chiropractic care can address by restoring balance (Abitbol, 1987).
Foley, B. S., & Buschbacher, R. M. (2014). Sacroiliac joint pain: Anatomy, biomechanics, diagnosis, and treatment. American Journal of Physical Medicine & Rehabilitation, 93(8), 687-697. https://pubmed.ncbi.nlm.nih.gov/15213481/
Sarkari, E., et al. (2023). Effect of hip joint mobilisations and strength training on pain, physical function and dynamic balance in patients with knee osteoarthritis: A randomized controlled trial. Journal of Bodywork and Movement Therapies, 35, 340-347. https://pubmed.ncbi.nlm.nih.gov/37330770/
Hogston, P. (2015). The evolution of the human pelvis: Changing adaptations to bipedalism, obstetrics and thermoregulation. Philosophical Transactions of the Royal Society B: Biological Sciences, 370(1663), 20140063. https://pubmed.ncbi.nlm.nih.gov/25602067/
Abitbol, M. M. (1987). Anatomy and clinical significance of sacral variations: A systematic review. Clinical Anatomy, 30(5), 646-655. https://pubmed.ncbi.nlm.nih.gov/28508536/
Teamwork Makes the Dream Work: Integrating Therapies
At ChiroMed, Dr. Jimenez leads a monster squad of professionals to help you recover. Chiropractic care is often paired with:
Physical Therapy: To strengthen muscles and improve movement, reducing stress on the SI joint and hips (Binns Family Chiropractic, 2024).
Acupuncture: To ease pain and boost healing by hitting key points (El Paso Back Clinic, n.d.).
Nutrition Counseling: To fight inflammation with a diet as wholesome as Lily’s cooking (ChiroMed – Integrated Medicine, n.d.).
Functional Medicine: To tackle systemic issues like hormonal imbalances or gut health that might contribute to pain (Jimenez, n.d.).
This integrated approach is like assembling a team of ghouls to clean up a haunted house—each brings a unique skill to get the job done!
Let’s set aside the Herman Munster antics for a moment and get serious. Sacroiliac joint dysfunction and hip pain can significantly impact your daily life, but chiropractic care, led by Dr. Alexander Jimenez at ChiroMed – Integrated Medicine in El Paso, TX, offers a proven, non-invasive solution. By addressing the root causes of pain through adjustments, rehab exercises, and a holistic approach, Dr. Jimenez helps patients regain mobility, reduce discomfort, and live fuller lives.
For personal injury cases, Dr. Jimenez’s dual expertise as a chiropractor and nurse practitioner, combined with advanced imaging and diagnostics, makes him a trusted partner for recovery and legal documentation. His comprehensive care ensures you heal while supporting your case with detailed medical reports.
Disclaimer: This blog post is for informational purposes only and is not a substitute for professional medical advice. Always consult a qualified healthcare provider, such as Dr. Alex Jimenez, DC, APRN, FNP-BC, for a proper diagnosis and personalized treatment plan. The information provided is based on evidence-based research and clinical insights but should not be taken as medical advice without professional consultation. For more information or to schedule a visit, contact ChiroMed – Integrated Medicine at +1 (915) 412-6680 or [email protected].
Hogston, P. (2015). The evolution of the human pelvis: Changing adaptations to bipedalism, obstetrics and thermoregulation. Philosophical Transactions of the Royal Society B: Biological Sciences, 370(1663), 20140063. https://pubmed.ncbi.nlm.nih.gov/25602067/
Abitbol, M. M. (1987). Anatomy and clinical significance of sacral variations: A systematic review. Clinical Anatomy, 30(5), 646-655. https://pubmed.ncbi.nlm.nih.gov/28508536/
Foley, B. S., & Buschbacher, R. M. (2014). Sacroiliac joint pain: Anatomy, biomechanics, diagnosis, and treatment. American Journal of Physical Medicine & Rehabilitation, 93(8), 687-697. https://pubmed.ncbi.nlm.nih.gov/15213481/
Krishnamurthy, V., et al. (2020). Chronic hip pain in adults: Current knowledge and future prospective. Journal of Anaesthesiology Clinical Pharmacology, 36(Suppl 1), S56-S61. https://pubmed.ncbi.nlm.nih.gov/33100663/
Sarkari, E., et al. (2023). Effect of hip joint mobilisations and strength training on pain, physical function and dynamic balance in patients with knee osteoarthritis: A randomized controlled trial. Journal of Bodywork and Movement Therapies, 35, 340-347. https://pubmed.ncbi.nlm.nih.gov/37330770/
Introduction: Why Spinal Health Matters for Digestion
When most people think about digestive issues like bloating or constipation, they often imagine dietary triggers—too much dairy, not enough fiber, dehydration, or food sensitivities. While these are common causes, there’s another factor that’s frequently overlooked: spinal alignment.
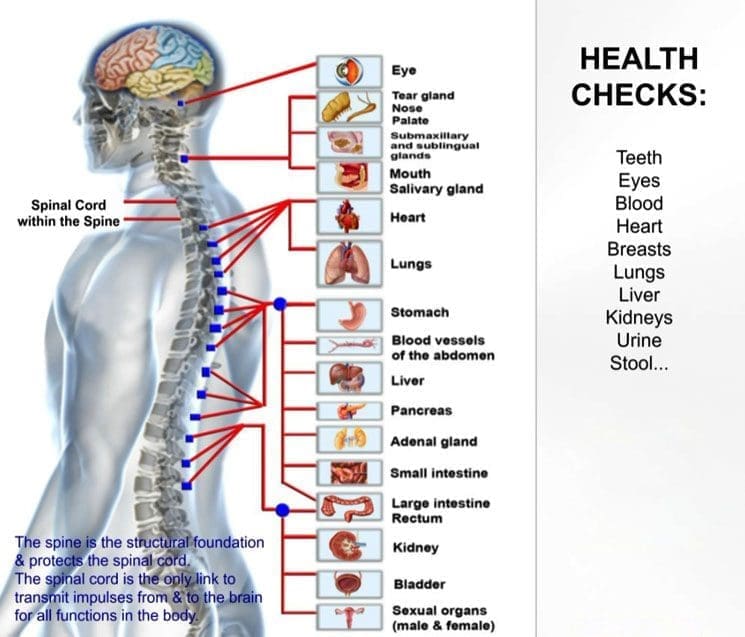
Your spine isn’t just a stack of bones that keeps you standing upright—it’s the protective housing for your spinal cord, a key part of your central nervous system (CNS). The CNS connects your brain to every organ in your body, including your stomach, intestines, and colon. If your spine is misaligned, it can disrupt the flow of nerve signals to your digestive organs, leading to discomfort, irregularity, and other gut-related symptoms (Medical News Today, n.d.).
This concept is not theoretical—it’s something chiropractors and integrative medicine practitioners see every day. A patient might come in for back pain but leave with improved digestion after their spinal alignment is corrected. The reason? Chiropractic care doesn’t just work on muscles and joints—it supports the nervous system, which in turn helps regulate digestive function (Bronson Heritage Chiropractic, n.d.).
Dr. Alexander Jimenez, DC, APRN, FNP-BC, a chiropractor and nurse practitioner in El Paso, has seen this connection in hundreds of patients. “When we restore proper spinal alignment,” he notes, “we’re not just improving posture—we’re improving communication between the brain and the rest of the body, and that includes the digestive system.”
How Spinal Misalignment Impacts Digestive Function
The digestive system works in a coordinated rhythm. Food moves from the stomach into the small intestine, where nutrients are absorbed, and then into the large intestine, where water is absorbed and waste is prepared for elimination. This process depends heavily on signals from the nervous system.
When vertebrae in your spine are out of place—what chiropractors call subluxations—the nerve signals between your brain and your digestive organs can be disrupted. For example:
Thoracic spine misalignments (mid-back) may affect the nerves that control the stomach and small intestine, leading to slowed digestion or bloating.
Lumbar spine misalignments (lower back) can interfere with nerve signals to the large intestine, potentially causing constipation.
Cervical spine misalignments (neck) may impact the vagus nerve, which plays a major role in digestion and gut motility.
When these nerves are compressed or irritated, they can send “mixed signals” to your gut. The result? Food might move too slowly, nutrients may not be absorbed efficiently, and bowel movements can become irregular (Spring Hill Premier Chiro, n.d.).
Dr. Jimenez points out that in many personal injury cases—especially after motor vehicle accidents—patients develop both musculoskeletal pain and unexplained digestive problems. Imaging often reveals spinal misalignments in the same areas that control digestive function. Correcting these issues can significantly improve both pain and gut symptoms.
Scientists and doctors often talk about the gut–brain axis—the constant communication between your brain and digestive system. However, the spinal cord also plays a crucial role in this process. Your brain sends messages to the gut through nerves that pass through the spine. If the spine is misaligned, it can distort or weaken those messages.
The vagus nerve, for example, helps regulate stomach acid production, muscle contractions in the intestines, and the release of digestive enzymes. A misalignment in the neck or upper back can irritate this nerve, leading to symptoms like heartburn, bloating, or sluggish digestion (Imagine Wellness Chiropractic, n.d.).
In Dr. Jimenez’s clinic, patients often report that, along with back pain relief, they notice better digestion after a few chiropractic sessions. This isn’t a coincidence—it’s the body functioning better because the nervous system is no longer being blocked by spinal misalignments (Thorburn Chiro, n.d.).
Bloating and Constipation: When the Spine Is the Culprit
Bloating and constipation are two of the most common digestive complaints in the United States. While dietary factors such as low fiber intake, dehydration, or excessive processed foods often play a role, spinal misalignment can be an under-recognized cause.
The lumbar spine—the lower portion of the back—is especially important for bowel function. Nerves that exit between the lumbar vertebrae communicate directly with the large intestine. If these vertebrae are misaligned, the nerve signals can be weakened or erratic. This disruption can slow down peristalsis, the wave-like muscle contractions that move food and waste through the intestines. Over time, this imbalance leads to constipation and the sensation of abdominal fullness or bloating (Gallatin Disc Center, n.d.).
It’s not just the lower spine that can play a role. The upper cervical spine—the top two vertebrae in the neck—can influence digestion via the vagus nerve. This nerve is a key component of the parasympathetic nervous system, which promotes “rest-and-digest” activity. Misalignment here can trigger issues like constipation, indigestion, and bloating (Roseville Blair Chiro, n.d.).
Dr. Jimenez recalls a patient—a 42-year-old office worker—who had suffered from chronic constipation for over five years. Despite dietary changes and over-the-counter remedies, her symptoms persisted. After a thorough examination, Dr. Jimenez identified misalignments in her lower lumbar spine and upper cervical region. Through a series of chiropractic adjustments and posture-corrective exercises, she experienced significant improvements in bowel regularity within two months.
Chiropractic care focuses on restoring proper spinal alignment, which in turn improves nerve communication between the brain and body. This is particularly important for digestive organs, which rely on constant, clear signals to regulate muscle movement, enzyme production, and fluid balance.
A chiropractic adjustment uses precise, gentle pressure to move misaligned vertebrae back into their correct position. This relieves nerve compression, restores normal motion to the spinal joints, and allows for better nervous system function. Over time, this improved communication can help reduce digestive symptoms such as bloating, constipation, reflux, and abdominal discomfort (Parc of Ontario, n.d.).
Many patients report positive digestive changes after beginning chiropractic care—even if they didn’t originally seek treatment for gut problems. One possible reason is that improved spinal alignment allows the parasympathetic nervous system to dominate, shifting the body away from chronic “fight or flight” stress mode and into “rest and digest” mode, which is essential for healthy bowel function (Artisan Chiro Clinic, n.d.).
Dr. Jimenez frequently integrates chiropractic care with nutritional recommendations and ergonomic advice for patients whose digestive symptoms are linked to poor posture at work. This combination not only addresses spinal misalignment but also prevents future nerve irritation from recurring workplace habits.
Integrative Medicine and Gut Health
The gut is influenced by multiple factors—diet, hydration, stress, posture, and physical activity all play major roles. Dr. Jimenez’s integrative medicine approach considers all these elements. He often incorporates:
Nutritional Counseling: Focusing on anti-inflammatory foods and adequate fiber intake to support bowel regularity.
Stress Management: Teaching breathing exercises and mindfulness techniques to reduce nervous system tension, which can slow digestion.
Postural Training: Helping patients adjust workstations and daily habits to minimize spinal strain.
Rehabilitation Exercises: Strengthening core muscles to support proper spinal alignment and protect nerve function.
Scientific evidence supports this multifaceted strategy. A healthy diet can reduce gut inflammation, restore a balanced microbiome, and support optimal nerve function (Dr. Schaer Institute, n.d.).
Patients who combine chiropractic adjustments with lifestyle changes often experience faster and more lasting relief compared to those who rely on a single intervention.
Rehabilitation Strategies for Long-Term Health
Chiropractic care can be the cornerstone of a digestive health plan, but it works best when paired with other rehabilitation strategies:
Targeted Exercise: Strengthens spinal support muscles, reducing the risk of misalignment and nerve irritation.
Massage Therapy: Relieves muscle tension that can pull the spine out of alignment and indirectly affect nerve pathways to the gut.
Acupuncture: Can stimulate nerve function, improve blood flow to digestive organs, and help regulate bowel movements.
Lifestyle Coaching: Guides patients in making daily choices that support both spinal and gut health, such as proper lifting techniques and balanced meal planning.
This combined approach helps patients maintain spinal stability, reduces inflammation, and keeps the nervous system functioning optimally (Dallas Accident and Injury Rehab, n.d.).
Dr. Jimenez stresses that rehabilitation is not a “quick fix”—it’s a long-term commitment to body alignment and nervous system health. His treatment plans often include re-evaluations every few weeks, with imaging or orthopedic testing to confirm progress.
Conclusion
Spinal misalignment can cause far more than back and neck pain—it can disrupt the nerve pathways that control digestion, leading to bloating, constipation, and other gut health problems. Chiropractic care addresses these root causes by restoring alignment and optimizing nervous system function.
When combined with integrative medicine strategies—nutrition, exercise, stress management, and targeted therapies like massage or acupuncture—patients can achieve better digestive function and improved overall health.
Dr. Alexander Jimenez’s dual role as a chiropractor and nurse practitioner allows him to bridge medical and biomechanical care, providing thorough diagnostic evaluation, effective spinal treatment, and the ability to handle legal documentation for personal injury cases. His approach ensures that patients recover fully—not just symptomatically—by addressing the underlying causes of both spinal and digestive issues.
Learn about the benefits of chiropractic care in treating piriformis syndrome discomfort and restoring movement.
Understanding Piriformis Syndrome and the Power of Chiropractic Care
If you’ve ever felt a sharp twinge in your backside that makes sitting through a movie or climbing stairs feel like a Herculean task, you might be dealing with piriformis syndrome. This pesky condition can turn your daily routine into a literal pain in the butt, but don’t worry—there’s hope! Chiropractic care, especially from experts like Dr. Alexander Jimenez in El Paso, TX, can help you kick that pain to the curb and get back to living your best life. In this comprehensive guide, we’ll break down what piriformis syndrome is, how it differs from its sneaky doppelgänger sciatica, and why chiropractic care is a superhero in the fight against musculoskeletal pain. Plus, we’ll explore how Dr. Jimenez’s unique expertise makes him a go-to for personal injury cases in El Paso. So, grab a comfy seat (or maybe stand for now), and let’s dive in with a dash of humor to keep things light!
What Is Piriformis Syndrome? Meet Your Butt’s Grumpy Neighbor
Picture this: a small, pear-shaped muscle called the piriformis, tucked away in your gluteal region, decides to throw a tantrum. This muscle, which runs from your sacrum (that triangular bone at the base of your spine) to the top of your femur (thigh bone), is usually a team player, helping you rotate your hip and move your leg. But when it gets irritated, tight, or inflamed, it can pinch the sciatic nerve—the body’s largest nerve, which runs right nearby. The result? Piriformis syndrome, a condition that feels like your backside is staging a protest.
Piriformis syndrome causes pain, numbness, or tingling in the buttocks, often radiating down the back of your leg. It’s like your body’s way of saying, “Hey, I’m not happy about all that sitting or sprinting you’ve been doing!” The pain can flare up during activities like sitting for too long, climbing stairs, or trying to channel your inner track star. Research suggests that piriformis syndrome accounts for 6–8% of sciatica-like symptoms not caused by a herniated disc (Jankovic et al., 2013).
Symptoms of Piriformis Syndrome
Here’s what you might experience when your piriformis muscle is in a bad mood:
Buttock pain: A deep, aching sensation that makes sitting feel like you’re on a bed of nails.
Radiating discomfort: Pain, numbness, or tingling that travels down your thigh, sometimes reaching your calf or foot.
Activity-related pain: Symptoms that worsen when you sit, stand, or move in certain ways, like crossing your legs or climbing stairs.
Tenderness: The piriformis muscle might feel sore when pressed, like a bruise you didn’t sign up for.
If this sounds like your daily struggle, don’t despair—chiropractic care can help, and we’ll get to that soon. But first, let’s clear up the confusion between piriformis syndrome and sciatica, because these two are like twins who keep getting mistaken for each other.
References:
Jankovic, D., Peng, P., & van Zundert, A. (2013). Piriformis syndrome: A cause of nondiscogenic sciatica. Current Pain and Headache Reports, 17(9), 355. https://pubmed.ncbi.nlm.nih.gov/23934706/
Piriformis Syndrome vs. Sciatica: Same Same, But Different
Piriformis syndrome and sciatica are like those celebrity look-alikes who get mobbed by paparazzi for all the wrong reasons. They share similar symptoms, but their causes and treatments can differ significantly. Let’s break it down so you can spot the differences and avoid treating the wrong culprit.
What Is Sciatica?
Sciatica is pain that follows the path of the sciatic nerve, which stretches from your lower back through your hips, buttocks, and down each leg. It’s typically caused by compression or irritation of the sciatic nerve roots, often due to spinal issues like a herniated disc, spinal stenosis, or degenerative disc disease. The pain can range from a mild ache to a fiery burn, usually affecting one side of the body.
Similarities Between Piriformis Syndrome and Sciatica
Both conditions can make you rethink your life choices every time you sit down. Here’s how they overlap:
Radiating pain: Both cause pain, numbness, or tingling that starts in the buttocks and travels down the leg, following the sciatic nerve’s path.
Worsened by sitting: Long periods of sitting can aggravate symptoms, turning your cozy couch into a torture device.
Muscle involvement: Tight or weak muscles in the hip or lower back can contribute to both conditions, making them partners in crime.
Key Differences
Despite their similarities, piriformis syndrome and sciatica have distinct characteristics:
Cause: Sciatica is typically caused by a spinal issue, like a herniated disc pressing on the sciatic nerve roots. Piriformis syndrome occurs when the piriformis muscle itself compresses the sciatic nerve, often without any spinal involvement (Hicks et al., 2021).
Pain location: Sciatica pain often starts in the lower back and radiates downward. Piriformis syndrome pain usually originates in the buttocks and may not involve the lower back at all.
Diagnostic clues: Imaging tests like MRIs can identify spinal causes of sciatica, such as disc herniation. Piriformis syndrome is often diagnosed through physical exams, like the FAIR (flexion, adduction, internal rotation) test, which stretches the piriformis to reproduce symptoms (Siddiq et al., 2021).
Think of sciatica as a traffic jam caused by a roadblock in your spine, and piriformis syndrome as a jam caused by a tight muscle squeezing the nerve in your hip. Both slow you down, but the fix depends on where the problem starts.
Siddiq, M. A. B., Hossain, M. S., & Uddin, M. M. (2021). Surgical and Non-surgical Treatment Options for Piriformis Syndrome: A Literature Review. Cureus, 13(3), e13953. https://pubmed.ncbi.nlm.nih.gov/33927967/
Musculoskeletal Pain: The Root of the Problem
Musculoskeletal pain is like that uninvited guest who shows up to your party, eats all the snacks, and refuses to leave. It affects your muscles, bones, ligaments, tendons, or nerves, and it’s a major player in conditions like piriformis syndrome. Understanding how musculoskeletal pain contributes to piriformis syndrome is key to finding lasting relief.
Causes of Musculoskeletal Pain in Piriformis Syndrome
The piriformis muscle can get cranky for a variety of reasons, many of which overlap with general musculoskeletal pain triggers:
Overuse or strain: Repetitive activities like running, cycling, or sitting for hours can overwork the piriformis, leading to tightness or spasms (Jimenez, 2023).
Poor posture: Slouching at your desk or hunching over your phone can stress the piriformis and surrounding muscles.
Muscle imbalances: Weak glutes or tight hip flexors can force the piriformis to pick up the slack, causing irritation.
Trauma or injury: A fall, car accident, or sports mishap can injure the piriformis or nearby tissues, leading to inflammation and nerve compression (Cedars-Sinai, n.d.).
Sedentary lifestyle: Too much sitting weakens the muscles supporting your pelvis, making the piriformis more prone to tightness.
These factors create a perfect storm for musculoskeletal pain, which can manifest as piriformis syndrome when the muscle compresses the sciatic nerve. The pain can also spread to nearby areas, like the lower back or thighs, making it feel like your entire lower body is staging a revolt.
Overlapping Risk Profiles
Piriformis syndrome shares risk factors with other musculoskeletal conditions, meaning tackling it can help prevent a host of related issues. Common risk factors include:
Sedentary behavior: Prolonged sitting weakens the glutes and tightens the hip flexors, increasing the risk of piriformis syndrome and lower back pain (Bordoni & Varacallo, 2021).
Repetitive stress: Athletes or workers who perform repetitive motions (think runners or warehouse workers) are more likely to develop piriformis syndrome and other overuse injuries.
Poor core stability: Weak core muscles can lead to improper pelvic alignment, contributing to piriformis syndrome and nonspecific low back pain (Lee et al., 2020).
Previous injuries: Trauma, like a car accident or fall, can predispose you to musculoskeletal pain and piriformis syndrome, especially if scar tissue or muscle imbalances develop.
Addressing these risk factors not only helps manage piriformis syndrome but also reduces your chances of developing related conditions like chronic low back pain or hip dysfunction.
Bordoni, B., & Varacallo, M. (2021). Extra-spinal sciatica and sciatica mimics: A scoping review. Korean Journal of Pain, 34(1), 12–22. https://pubmed.ncbi.nlm.nih.gov/33380567/
Lee, J. H., Kim, S. H., & Park, S. H. (2020). Core Stability and Hip Exercises Improve Physical Function and Activity in Patients with Non-Specific Low Back Pain: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 17(15), 5423. https://pubmed.ncbi.nlm.nih.gov/32731549/
Chiropractic Care: Your Superhero for Piriformis Syndrome
Now, let’s talk about the hero of this story: chiropractic care. It’s like sending in a skilled mechanic to fix your body’s misaligned gears and soothe those cranky muscles. Chiropractors, like Dr. Alexander Jimenez, use a combination of adjustments, manual therapies, and rehabilitation exercises to tackle piriformis syndrome and help you regain mobility.
Why Chiropractic Care Works
Chiropractic care is a powerhouse for piriformis syndrome because it addresses both the musculoskeletal and neurological components of the condition. Here’s the clinical rationale:
Spinal and pelvic alignment: Misalignments in the spine or pelvis can contribute to piriformis tightness by altering muscle and nerve interactions. Chiropractic adjustments restore proper Atsumari alignment, reducing pressure on the sciatic nerve (Jimenez, 2023).
Muscle relaxation: Techniques like myofascial release and soft tissue therapy loosen the piriformis muscle, relieving its chokehold on the sciatic nerve (Siddiq et al., 2021).
Improved mobility: Chiropractors prescribe stretching and strengthening exercises to enhance hip and pelvic mobility, preventing future flare-ups (Tonley et al., 2010).
Holistic approach: Chiropractic care includes lifestyle advice, like posture correction and ergonomic tips, to tackle the root causes of musculoskeletal pain.
It’s like a three-pronged attack: adjustments fix the structure, therapies calm the muscles, and exercises build a stronger foundation. Together, they send piriformis syndrome running for the hills.
Evidence-Based Benefits
Research backs up the effectiveness of chiropractic and related therapies for piriformis syndrome. A study found that sciatic nerve mobilization and piriformis muscle release significantly reduced pain and improved function in patients with piriformis syndrome (Santos et al., 2022). Another study showed that core stability and hip exercises improved physical function in patients with musculoskeletal pain, aligning with the chiropractic approach to correcting muscle imbalances (Lee et al., 2020).
Siddiq, M. A. B., Hossain, M. S., & Uddin, M. M. (2021). Surgical and Non-surgical Treatment Options for Piriformis Syndrome: A Literature Review. Cureus, 13(3), e13953. https://pubmed.ncbi.nlm.nih.gov/33927967/
Tonley, J. C., Yun, S. M., Kochevar, R. J., Dye, J. A., Farrokhi, S., & Powers, C. M. (2010). Treatment of an individual with piriformis syndrome using a multimodal approach including joint mobilization, soft tissue techniques, and exercise. Journal of Orthopaedic & Sports Physical Therapy, 40(2), 92–98.
Santos, F. M., da Silva, J. T., & de Souza, P. B. (2022). Physiotherapy for Piriformis Syndrome Using Sciatic Nerve Mobilization and Piriformis Release. Journal of Bodywork and Movement Therapies, 29, 135–140. https://pubmed.ncbi.nlm.nih.gov/35114532/
Lee, J. H., Kim, S. H., & Park, S. H. (2020). Core Stability and Hip Exercises Improve Physical Function and Activity in Patients with Non-Specific Low Back Pain: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 17(15), 5423. https://pubmed.ncbi.nlm.nih.gov/32731549/
Vij, N., Kiernan, H., Bisht, R., Singleton, I., Cornett, E. M., Kaye, A. D., … & Urits, I. (2021). Surgical and non-surgical treatment options for piriformis syndrome: A literature review. Anesthesia & Pain Medicine, 11(1), e112825. https://doi.org/10.5812/aapm.112825
Piriformis Syndrome Treatment- Video
Dr. Alexander Jimenez: El Paso’s Personal Injury and Pain Expert
If you’re in El Paso and grappling with piriformis syndrome or a personal injury, Dr. Alexander Jimenez is the practitioner you want on your team. As a board-certified Family Practice Nurse Practitioner (FNP-C) and Chiropractor (DC), Dr. Jimenez combines chiropractic expertise with advanced medical diagnostics, making him a standout at ChiroMed – Integrated Medicine. His unique skill set and holistic approach make him a trusted ally for patients seeking relief and recovery.
Advanced Imaging and Diagnostics
Dr. Jimenez uses cutting-edge tools to get to the root of your pain:
MRI or CT scans: To rule out spinal causes of sciatica and confirm piriformis involvement.
Electromyography (EMG): To assess nerve function and detect sciatic nerve irritation.
Physical exams: Tests like the FAIR test or Pace sign to pinpoint piriformis-specific pain (Jankovic et al., 2013).
These diagnostics ensure that treatment is targeted and effective, addressing the real cause of your discomfort.
Dual-Scope Procedures
Dr. Jimenez’s dual training allows him to bridge conservative and medical care. His approach includes:
Chiropractic adjustments: To correct spinal and pelvic misalignments that contribute to piriformis syndrome.
Soft tissue therapies: Like myofascial release to relax the piriformis and reduce nerve compression.
Rehabilitation exercises: Customized stretches and strengthening routines to restore balance and prevent recurrence.
This integrated approach ensures comprehensive care that tackles both immediate pain and long-term recovery.
Supporting Personal Injury Cases
In El Paso, personal injury cases—such as those from car accidents or workplace incidents—are common, and Dr. Jimenez excels at supporting victims. He provides detailed medical documentation that links injuries to the incident, crucial for legal claims. His expertise in advanced imaging and diagnostics allows him to identify injuries like piriformis syndrome or spinal misalignments caused by trauma, offering clear evidence for attorneys and insurance companies. This makes him an invaluable liaison between medical care and legal proceedings, helping patients achieve both healing and justice.
References:
Jankovic, D., Peng, P., & van Zundert, A. (2013). Piriformis syndrome: A cause of nondiscogenic sciatica. Current Pain and Headache Reports, 17(9), 355. https://pubmed.ncbi.nlm.nih.gov/23934706/
Changing Your Daily Routine to Prevent Piriformis Syndrome
Prevention is better than a cure, especially when your piriformis is acting like a grumpy cat. Making small changes to your daily routine can reduce your risk of piriformis syndrome and other musculoskeletal issues. Here are some practical, evidence-based tips:
1. Move More, Sit Less
Sitting for hours is the piriformis muscle’s kryptonite. Try these:
Take breaks: Stand, stretch, or walk every 30–60 minutes to keep your hips happy.
Use a standing desk: Alternate between sitting and standing to reduce pressure on the piriformis.
Try active sitting: Use an exercise ball or ergonomic chair to engage your core and minimize strain.
2. Stretch and Strengthen
Incorporate exercises to keep your piriformis and surrounding muscles in check:
Piriformis stretch: Lie on your back, cross one ankle over the opposite knee, and pull the thigh toward your chest. Hold for 20–30 seconds per side (Santos et al., 2022).
Glute bridges: Strengthen your glutes to reduce strain on the piriformis. Aim for 2–3 sets of 10–15 reps.
Core exercises: Planks or bird-dog exercises improve pelvic stability, reducing the risk of muscle imbalances (Lee et al., 2020).
3. Mind Your Posture
Poor posture is like inviting piriformis syndrome to a sleepover. Try these:
Sit smart: Keep your feet flat, knees at 90 degrees, and back straight.
Sleep right: Avoid sleeping on your side with your top leg crossed over, as it can tighten the piriformis.
Lift properly: Bend at the knees, not the waist, to avoid stressing your lower back and hips.
4. Incorporate Yoga
Yoga is a fun way to keep your hips and back happy. Poses like the pigeon pose or the child’s pose target the piriformis and improve flexibility. A study on yoga for dental professionals (who sit a lot, like many of us) found that specific poses reduced musculoskeletal pain and improved function (Gandolfi et al., 2023).
5. See a Chiropractor Regularly
Regular chiropractic visits can catch potential issues before they become major problems. Dr. Jimenez’s holistic approach at ChiroMed includes preventive care, such as adjustments and lifestyle advice, to keep your musculoskeletal system in top shape.
By making these changes, you’re not just dodging piriformis syndrome—you’re building a stronger, more resilient body ready to tackle life’s challenges (except maybe a surprise marathon).
References:
Santos, F. M., da Silva, J. T., & de Souza, P. B. (2022). Physiotherapy for Piriformis Syndrome Using Sciatic Nerve Mobilization and Piriformis Release. Journal of Bodywork and Movement Therapies, 29, 135–140. https://pubmed.ncbi.nlm.nih.gov/35114532/
Lee, J. H., Kim, S. H., & Park, S. H. (2020). Core Stability and Hip Exercises Improve Physical Function and Activity in Patients with Non-Specific Low Back Pain: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 17(15), 5423. https://pubmed.ncbi.nlm.nih.gov/32731549/
Gandolfi, M. G., Zamparini, F., Spinelli, A., & Prati, C. (2023). Āsana for Back, Hips, and Legs to Prevent Musculoskeletal Disorders among Dental Professionals: In-Office Yóga Protocol. International Journal of Yoga, 16(1), 10–17. https://pubmed.ncbi.nlm.nih.gov/37583546/
A Light-Hearted Look at Living Pain-Free
Dealing with piriformis syndrome can feel like your backside is holding a grudge, but with chiropractic care and a few lifestyle tweaks, you can send that pain packing. Imagine a world where sitting through a meeting doesn’t require a strategic cushion or where climbing stairs doesn’t feel like a mission to Mars. That’s the world Dr. Alexander Jimenez and his team at ChiroMed are helping patients achieve every day.
Whether you’re an athlete sidelined by pain, a desk warrior battling the effects of too many Zoom calls, or a personal injury victim seeking healing and justice, chiropractic care offers a path to relief that’s both effective and empowering. So, why not give your piriformis a break and let the experts guide you back to a pain-free life?
Conclusion: A Serious Note
While we’ve had some fun exploring the quirks of piriformis syndrome, this condition is no laughing matter. It can significantly impact your quality of life, and untreated musculoskeletal pain may lead to chronic issues or complications. Seeking professional care from a qualified practitioner like Dr. Alexander Jimenez, DC, APRN, FNP-C, is essential for accurate diagnosis and effective treatment. His expertise in chiropractic care, advanced diagnostics, and personal injury support makes him a trusted resource for El Paso residents.
Disclaimer: The information in this blog post is for educational purposes only and is not intended to replace professional medical advice. Always consult a qualified healthcare provider for personalized diagnosis and treatment plans tailored to your specific needs. For more information or to schedule a consultation, contact ChiroMed – Integrated Medicine at +1 (915) 412-6680 or [email protected].
Gandolfi, M. G., Zamparini, F., Spinelli, A., & Prati, C. (2023). Āsana for Back, Hips, and Legs to Prevent Musculoskeletal Disorders among Dental Professionals: In-Office Yóga Protocol. International Journal of Yoga, 16(1), 10–17. https://pubmed.ncbi.nlm.nih.gov/37583546/
At ChiroMed – Integrated Medicine in El Paso, TX, we believe in addressing the root causes of health issues to promote holistic healing. A key factor in musculoskeletal health and injury recovery is the gut microbiome, a complex community of microorganisms in your digestive tract. These tiny organisms play a significant role in supporting muscle growth, bone health, and recovery from injuries by regulating simplified nutrient absorption, modulating inflammation, and influencing hormone production. However, an imbalance in the gut, known as dysbiosis, can hinder these processes and contribute to musculoskeletal problems. At ChiroMed, we integrate this cutting-edge science into our personalized treatment plans to help you achieve optimal health.
How the Gut Supports Nutrient Absorption
The gut microbiome is essential for absorbing nutrients that keep your muscles and bones strong. Calcium and vitamin D, critical for bone health, are better absorbed when gut bacteria are balanced (Hsu et al., 2024). These microbes break down food, ensuring your body receives the nutrients it needs for skeletal strength and muscle repair. Short-chain fatty acids (SCFAs), produced by gut bacteria, also enhance bone density, supporting long-term skeletal health without relying solely on supplements (Li et al., 2021).
For muscles, the gut ensures proteins and amino acids are absorbed efficiently, fueling growth and repair after exercise or injury (Harvard Medical School, 2023). At ChiroMed, our nutrition counseling services focus on optimizing gut health to maximize nutrient uptake, helping you build stronger muscles and bones naturally.
Inflammation is a natural part of healing, but excessive inflammation can slow recovery and increase pain. A healthy gut microbiome produces metabolites like SCFAs that reduce inflammation, creating an optimal environment for muscle and bone repair (West Limerick Physiotherapy, 2023). This helps patients at ChiroMed recover faster from injuries, whether from sports, work, or accidents.
When the gut is imbalanced, chronic inflammation can delay healing and worsen musculoskeletal conditions (AstonRX, 2023). Our integrative approach at ChiroMed, including acupuncture and naturopathy, supports gut health to keep inflammation in check, promoting quicker recovery and less pain.
The gut microbiome influences hormone production, which is vital for muscle and bone health. For example, gut bacteria regulate insulin-like growth factor 1 (IGF-1), a hormone that supports muscle growth and repair (Grosicki et al., 2021). A balanced gut also enhances hormonal pathways for calcium metabolism, strengthening bones over time (Yan et al., 2023).
Dysbiosis can disrupt these hormones, leading to weaker muscles and bones, and slower recovery (IAOM-US, 2023). At ChiroMed, our team, led by Dr. Alex Jimenez, incorporates nutrition and integrative medicine to support gut health, ensuring hormones work in your favor for optimal musculoskeletal function.
A healthy gut microbiome supports muscle growth by improving nutrient absorption and reducing inflammation, providing the energy and materials needed for repair (MyProtein, 2023). For bones, gut bacteria enhance calcium and vitamin D uptake, while probiotics can reduce bone loss, especially in conditions like osteoporosis (Taylor & Francis, 2024). At ChiroMed, our rehabilitation programs and chiropractic care work alongside gut-focused nutrition plans to strengthen muscles and bones, helping you stay active and resilient.
The gut microbiome supports injury recovery by reducing inflammation and supplying nutrients for tissue repair (Harvard Medical School, 2023). Gut microbes produce compounds that speed up muscle regeneration, helping you recover faster from sprains, fractures, or strains (Digbi Health, 2023). At ChiroMed, our team uses advanced diagnostics, like X-rays and MRIs, to assess injuries accurately and create tailored recovery plans that incorporate gut health strategies.
An imbalanced gut, however, can slow healing by causing chronic inflammation and nutrient deficiencies (Healio, 2023). Our holistic approach at ChiroMed addresses these issues, combining chiropractic adjustments, massage therapy, and nutrition to
Dysbiosis, or an unhealthy gut microbiome, can disrupt nutrient absorption, increase inflammation, and throw off hormone balance, all of which harm musculoskeletal health (PMC, 2024). This can lead to slower recovery, weaker bones, and increased risk of injuries like fractures (ScienceDirect, 2023). At ChiroMed, we use nutrition counseling and naturopathy to restore gut balance, helping prevent these issues and support long-term wellness.
Dr. Alex Jimenez, DC, APRN, FNP-C, leads ChiroMed with a unique blend of chiropractic and nurse practitioner expertise. Specializing in work, sports, personal, and auto accident injuries, Dr. Jimenez uses advanced imaging and diagnostic tools to create precise, dual-scope diagnoses (Jimenez, 2023a). His ability to handle medical care and legal paperwork for personal injury cases ensures patients receive comprehensive support, from treatment to insurance claims (Jimenez, 2023b).
At ChiroMed, our integrated approach combines chiropractic care, massage therapy, acupuncture, naturopathy, and nutrition counseling to address a wide range of injuries. Chiropractic adjustments restore joint and spine alignment, reducing pain and improving mobility. Massage therapy eases muscle tension, while acupuncture promotes natural healing by targeting pain points. Our nutrition and naturopathy services focus on gut health to reduce inflammation and enhance recovery, preventing long-term complications (Jimenez, 2023c). This comprehensive care ensures patients return to optimal health naturally.
The gut microbiome is a powerful ally in musculoskeletal health and injury recovery, influencing nutrient absorption, inflammation, and hormone production. At ChiroMed – Integrated Medicine, we harness this science through personalized, holistic care to help you heal faster and stay stronger. By combining chiropractic care, integrative medicine, and gut-focused nutrition, we address the root causes of injuries and promote long-term wellness. Visit ChiroMed in El Paso, TX, to experience how our integrated approach can transform your health.
Grosicki, G. J., Fielding, R. A., & Lustgarten, M. S. (2021). The gut microbiota interacts with the musculoskeletal system and can affect muscle growth and development. Nutrients, 13(6), Article 1917. https://pmc.ncbi.nlm.nih.gov/articles/PMC9132697/
Yan, J., Herzog, J., & Tsang, K. (2023). The interaction between GM and dietary minerals are crucial for bone mineralization. Nutrients, 15(9), Article 2066. https://pmc.ncbi.nlm.nih.gov/articles/PMC11062616/
Learn the benefits of calisthenics and chiropractic care for athletes looking to improve performance and reduce injury risks.
Chiropractic Care and Calisthenics: A Dynamic Duo for Musculoskeletal Pain Relief in El Paso
Musculoskeletal pain is a pesky problem that can turn your daily routine into a real pain in the neck—literally! Whether it’s a nagging backache, a stiff neck, or sore joints, this discomfort can stem from injuries, poor posture, or just sitting at a desk all day, dreaming of tacos. In El Paso, TX, ChiroMed – Integrated Medicine, led by the talented Dr. Alex Jimenez, DC, APRN, FNP-C, offers a game-changing solution by combining chiropractic care with calisthenics, a bodyweight exercise method with roots in ancient Greece. This blog post dives deep into why this combo is a powerhouse for reducing musculoskeletal pain and its overlapping risk factors, provides easy calisthenic exercises you can do anywhere, and highlights Dr. Jimenez’s expertise in personal injury cases. With a dash of humor to keep things light, let’s explore how you can kick pain to the curb and feel like a superhero in no time!
What Is Musculoskeletal Pain and Why Should You Care?
Musculoskeletal pain affects the muscles, bones, joints, ligaments, tendons, or nerves, making everyday tasks like lifting groceries or chasing your dog feel like an Olympic event. It’s a widespread issue, with chronic pain impacting millions and costing billions in healthcare and lost productivity (Gatchel et al., 2020). The causes are as varied as the toppings on an El Paso taco:
Injuries: Sprains, strains, or trauma from car accidents, sports, or slipping on that sneaky patch of ice.
Chronic Conditions: Think fibromyalgia, arthritis, or sciatica that just won’t quit.
Lifestyle Habits: Hours of Netflix binging or slouching at a desk can wreak havoc on your spine.
Stress and Anxiety: These can tighten muscles faster than you can say “deadline.”
These factors don’t just work alone—they team up like a gang of troublemakers, creating overlapping risk profiles that make pain worse. For example, sitting too long weakens your core, which messes with your posture, which then gets aggravated by stress-induced muscle tension. It’s like a bad sitcom rerun you can’t escape.
The good news? Chiropractic care and calisthenics can break this cycle. Chiropractic adjustments fix spinal misalignments and ease nerve pressure, while calisthenics strengthen muscles and boost mobility. Together, they tackle the root causes of pain and reduce risks like weak muscles, poor posture, and inflammation, helping you move better and feel better.
References
Gatchel, R. J., Reuben, D. B., Dagenais, S., Turk, D. C., Chou, R., Hershey, A. D., … & Horn, S. D. (2020). Chronic musculoskeletal pain: Nonpharmacologic, noninvasive treatments. American Family Physician, 102(8), 465–472. Retrieved from https://pubmed.ncbi.nlm.nih.gov/33064420/
The Magic of Chiropractic Care
At ChiroMed – Integrated Medicine in El Paso, chiropractic care is the star of the show, and Dr. Alex Jimenez is the director. With over 20 years of experience since graduating from the University of Vermont in 1999, Dr. Jimenez blends chiropractic expertise with his skills as a family nurse practitioner to create personalized treatment plans that mix conventional and alternative medicine (ChiroMed – Integrated Medicine, n.d.).
How Does Chiropractic Care Help?
Chiropractic care focuses on fixing subluxations—misalignments in the spine or joints that irritate nerves, cause muscle tension, and limit movement. Through gentle spinal adjustments and manual therapy, chiropractors like Dr. Jimenez restore proper alignment, which is like hitting the reset button on your body’s control panel. This reduces pain, improves mobility, and helps your body function like a well-tuned machine.
Research backs this up big time. A systematic review found that combining manual therapy (like chiropractic adjustments) with exercise cuts pain and disability in people with nonspecific neck pain (Hidalgo et al., 2021). Here’s how chiropractic care tackles those overlapping risk factors:
Posture Power-Up: Adjustments correct spinal alignment, reducing strain on muscles and joints.
Mobility Boost: Restoring joint function makes it easier to move and exercise without wincing.
Inflammation Tamer: Proper alignment can dial down inflammation, helping your body chill out.
Dr. Jimenez’s Role in Personal Injury Cases
El Paso’s vibrant lifestyle—think hiking, sports, and busy roads—means personal injury cases like car accidents, workplace mishaps, or sports injuries are all too common. Dr. Jimenez shines as a go-to practitioner for these cases, thanks to his dual expertise as a chiropractor and nurse practitioner. His approach is like a superhero team-up, combining:
Advanced Imaging: Using X-rays, MRIs, or CT scans to spot injuries like herniated discs, whiplash, or soft tissue damage.
Thorough Diagnostics: Detailed assessments to understand the full extent of injuries and their impact.
Dual-Scope Care: Blending chiropractic adjustments with medical interventions like pain management or specialist referrals.
Legal Liaison: Providing clear, detailed medical reports for insurance claims or legal cases, ensuring patients get the care and compensation they need.
For example, if you’re in a fender-bender and end up with neck pain, Dr. Jimenez might use an MRI to diagnose a cervical subluxation, perform adjustments to fix it, and document everything for your lawyer. His work at ChiroMed makes him a trusted ally for El Pasoans navigating the aftermath of injuries (Jimenez, n.d.).
References
ChiroMed – Integrated Medicine. (n.d.). About us. Retrieved from https://chiromed.com/
Hidalgo, B., Hall, T., Bossert, J., Dugeny, A., Cagnie, B., & Pitance, L. (2021). The combined effects of manual therapy and exercise on pain and related disability for individuals with nonspecific neck pain: A systematic review with meta-analysis. Journal of Manual & Manipulative Therapy, 29(5), 260–271. Retrieved from https://pubmed.ncbi.nlm.nih.gov/34472424/
Calisthenics: Your Body’s Gym, No Membership Required
Calisthenics, from the Greek words for “beauty” and “strength,” is like the workout version of a Swiss Army knife—versatile, effective, and equipment-free. As detailed by El Paso Back Clinic, this ancient Greek training method builds strength, flexibility, and endurance using just your bodyweight, making it perfect for anyone looking to get fit and pain-free (El Paso Back Clinic, n.d.).
Why Calisthenics Rocks
You don’t need a fancy gym or weights that cost more than your rent. Calisthenics uses your body as resistance, so you can work out in your living room, backyard, or even while waiting for your coffee to brew. It targets multiple muscle groups, improves coordination, and boosts functional movement, all of which help reduce musculoskeletal pain. Studies show that bodyweight exercises like calisthenics are effective for chronic low back pain, improving core stability and reducing fatigue (Gordon & Bloxham, 2021; Owen et al., 2020).
Here’s why calisthenics is the perfect partner for chiropractic care:
Core Strength: A strong core supports your spine, reducing the risk of back pain.
Posture Perfection: Exercises like planks help you stand tall instead of slouching like a tired scarecrow.
Gordon, R., & Bloxham, S. (2021). Some types of exercise are more effective than others in people with chronic low back pain: A network meta-analysis. Journal of Physiotherapy, 67(4), 252–261. Retrieved from https://pubmed.ncbi.nlm.nih.gov/34580091/
Mace, C., Kerse, N., Maddison, R., Olds, T., Jatrana, S., Wham, C., … & Rolleston, A. (2022). The effect of breaking up sedentary time with calisthenics on neuromuscular function: A preliminary study. International Journal of Environmental Research and Public Health, 19(3), 1452. Retrieved from https://pubmed.ncbi.nlm.nih.gov/35162460/
Owen, P. J., Miller, C. T., Mundell, N. L., Verswijveren, S. J., Tagliaferri, S. D., Brisby, H., … & Belavy, D. L. (2020). Exercise therapy for chronic low back pain. Cochrane Database of Systematic Reviews, (9). Retrieved from https://pubmed.ncbi.nlm.nih.gov/32997745/
Five Calisthenic Exercises to Kick Pain to the Curb
Ready to get moving and tell pain to take a hike? Here are five beginner-friendly calisthenic exercises you can do at home or in a gym. They’re simple, effective, and require no gear—just your body and a bit of grit. (Note: Check with a pro like Dr. Jimenez before starting, especially if you have injuries or health conditions.)
1. Push-Ups (Chest, Shoulders, Core)
How to Do It: Get into a plank position with hands shoulder-width apart. Lower your chest toward the floor, keeping your body straight, then push back up. No face-planting, please!
Benefits: Builds upper body strength and core stability, reducing shoulder and neck pain.
Beginner Hack: Try knee push-ups if the full version feels like armageddon. You’ll still feel like a champ.
2. Bodyweight Squats (Legs, Glutes, Core)
How to Do It: Stand with feet hip-width apart. Lower your hips like you’re sitting in an invisible chair, keeping your chest up and knees over toes. Stand back up.
Benefits: Strengthens legs and glutes, supporting your lower back and improving posture.
Humor Alert: Pretend you’re dodging a swarm of bees—squat low and fast!
3. Plank (Core, Back, Shoulders)
How to Do It: Lie face down, then prop up on your forearms and toes, keeping your body straight like a board. Hold for 20–30 seconds or until you start dreaming of quitting.
Benefits: Boosts core strength, stabilizes the spine, and helps prevent lower back pain.
Beginner Tip: Start with 10-second holds. You’re not trying to break a world record… yet.
4. Lunges (Legs, Glutes, Core)
How to Do It: Step forward with one leg, lowering your back knee toward the ground. Keep your front knee over your ankle, then push back to start. Switch legs.
Benefits: Improves leg strength, balance, and hip flexibility, easing lower back strain.
Humor Alert: Imagine you’re lunging to grab the last slice of pizza—motivation matters!
5. Superman Hold (Back, Glutes, Core)
How to Do It: Lie face-down, arms extended overhead. Lift your arms, chest, and legs off the ground like you’re flying. Hold for 5–10 seconds, then lower.
Benefits: Strengthens your back and glutes, counteracting slouching and reducing back pain.
Beginner Tip: Lift just your arms or legs if the full move feels like you’re auditioning for a Marvel movie.
Sample 15-Minute Routine
Do this circuit 3–4 times a week:
Push-Ups: 10–15 reps
Bodyweight Squats: 15–20 reps
Plank: 20–30 seconds
Lunges: 10 reps per leg
Superman Hold: 5 reps (10 seconds each)
Pair this with chiropractic visits to ChiroMed for maximum results. Dr. Jimenez can check your form and tweak exercises to fit your needs, ensuring you’re not accidentally turning your workout into a comedy of errors.
Why Chiropractic Care and Calisthenics Are a Match Made in Heaven
Think of chiropractic care and calisthenics as peanut butter and jelly—they’re great on their own, but together, they’re unstoppable. Here’s how they team up to fight musculoskeletal pain and its pesky risk factors:
Fixing the Foundation: Chiropractic adjustments correct spinal and joint misalignments, setting the stage for effective exercise by reducing nerve irritation.
Building Strength: Calisthenics strengthens muscles, reinforcing the benefits of adjustments by stabilizing your spine and joints.
Pain Relief Powerhouse: Studies show that combining manual therapy with exercise is more effective than either alone for reducing pain and disability (Hidalgo et al., 2021).
Better Movement Control: Calisthenics improves neuromuscular stability, helping you move better and avoid re-injury (McCaskey et al., 2022).
Mental Health Bonus: Calisthenics can reduce stress and fatigue, which often worsen pain, making you feel as zen as a sunny El Paso afternoon (Niedermeier et al., 2021).
At ChiroMed, Dr. Jimenez crafts plans that blend these approaches. For instance, a patient with chronic back pain might get spinal adjustments to fix misalignments, followed by a calisthenics routine to strengthen their core, ensuring long-term relief and resilience.
References
Hidalgo, B., Hall, T., Bossert, J., Dugeny, A., Cagnie, B., & Pitance, L. (2021). The combined effects of manual therapy and exercise on pain and related disability for individuals with nonspecific neck pain: A systematic review with meta-analysis. Journal of Manual & Manipulative Therapy, 29(5), 260–271. Retrieved from https://pubmed.ncbi.nlm.nih.gov/34472424/
McCaskey, M. A., Wirth, B., & Balagué, F. (2022). The role of neuromuscular control of postural and core stability in functional movement and athlete performance. Frontiers in Physiology, 13, 796097. Retrieved from https://pubmed.ncbi.nlm.nih.gov/35250609/
Niedermeier, M., Fröhlich, K., Frühauf, A., & Kopp, M. (2021). Psychological effects of calisthenic exercises on neuroinflammatory and rheumatic diseases. Frontiers in Psychology, 12, 678075. Retrieved from https://pubmed.ncbi.nlm.nih.gov/34177728/
Personal Injury Care: Dr. Jimenez’s Expertise in El Paso
El Paso’s active vibe and busy streets mean personal injuries—like car crashes, workplace accidents, or sports mishaps—are part of life. Dr. Alex Jimenez at ChiroMed is a standout for these cases, thanks to his unique blend of chiropractic and medical expertise. His approach includes:
High-Tech Diagnostics: Using MRI, X-ray, or CT scans to pinpoint injuries like herniated discs or soft tissue damage.
Customized Treatment: Combining adjustments, rehabilitation, and calisthenics to restore function and ease pain.
Legal Support: Providing detailed medical reports for insurance or legal claims, ensuring patients get fair treatment.
Holistic Healing: Adding nutrition counseling, acupuncture, or naturopathy for complete recovery.
Imagine a patient with whiplash from a rear-end collision. Dr. Jimenez might use imaging to confirm a cervical issue, perform adjustments to restore alignment, and prescribe planks to strengthen neck muscles. His reports then help the patient’s lawyer build a strong case. This all-in-one approach makes Dr. Jimenez a vital resource for El Paso’s injury victims.
How to Add Chiropractic Care and Calisthenics to Your Life
Ready to ditch the pain and feel awesome? Here’s how to integrate chiropractic care and calisthenics into your routine, with a nod to Dr. Jimenez’s expertise:
Get Checked Out: Visit ChiroMed for a full assessment. Dr. Jimenez will spot any issues and create a custom plan.
Start with Adjustments: Regular chiropractic visits will fix misalignments and prep your body for exercise.
Add Calisthenics: Try the exercises above, aiming for 2–3 sessions a week. Focus on form to avoid looking like a wobbly Jenga tower.
Track Your Progress: Note changes in pain and mobility, and share them with Dr. Jimenez to fine-tune your plan.
Tweak Your Lifestyle: Sit less, stand taller, and chill out to keep those risk factors at bay.
A Pinch of Humor
Think of calisthenics as your body’s way of saying, “I’m ready to be awesome!” and chiropractic care as the coach that gets you there. So, put down the remote, crank up some music, and move like nobody’s watching—your spine will thank you!
Conclusion
Musculoskeletal pain doesn’t have to run your life. By combining chiropractic care and calisthenics, you can tackle pain, improve function, and reduce overlapping risk factors like weak muscles, poor posture, and stress. At ChiroMed – Integrated Medicine in El Paso, Dr. Alex Jimenez, DC, APRN, FNP-C, offers personalized care that blends spinal adjustments with exercises like push-ups and planks, helping patients achieve lasting relief. His expertise in personal injury cases, backed by advanced imaging and legal support, makes him a trusted partner for El Pasoans seeking recovery and justice.
Disclaimer: This blog post is for informational purposes only and is not a substitute for professional medical advice. Always consult a qualified healthcare provider, such as Dr. Alex Jimenez at ChiroMed – Integrated Medicine, before starting any exercise or treatment program. For personalized care, contact ChiroMed at +1 (915) 412-6680 or [email protected].
References
ChiroMed – Integrated Medicine. (n.d.). About us. Retrieved from https://chiromed.com/
Gatchel, R. J., Reuben, D. B., Dagenais, S., Turk, D. C., Chou, R., Hershey, A. D., … & Horn, S. D. (2020). Chronic musculoskeletal pain: Nonpharmacologic, noninvasive treatments. American Family Physician, 102(8), 465–472. Retrieved from https://pubmed.ncbi.nlm.nih.gov/33064420/
Hidalgo, B., Hall, T., Bossert, J., Dugeny, A., Cagnie, B., & Pitance, L. (2021). The combined effects of manual therapy and exercise on pain and related disability for individuals with nonspecific neck pain: A systematic review with meta-analysis. Journal of Manual & Manipulative Therapy, 29(5), 260–271. Retrieved from https://pubmed.ncbi.nlm.nih.gov/34472424/
Gordon, R., & Bloxham, S. (2021). Some types of exercise are more effective than others in people with chronic low back pain: A network meta-analysis. Journal of Physiotherapy, 67(4), 252–261. Retrieved from https://pubmed.ncbi.nlm.nih.gov/34580091/
Mace, C., Kerse, N., Maddison, R., Olds, T., Jatrana, S., Wham, C., … & Rolleston, A. (2022). The effect of breaking up sedentary time with calisthenics on neuromuscular function: A preliminary study. International Journal of Environmental Research and Public Health, 19(3), 1452. Retrieved from https://pubmed.ncbi.nlm.nih.gov/35162460/
McCaskey, M. A., Wirth, B., & Balagué, F. (2022). The role of neuromuscular control of postural and core stability in functional movement and athlete performance. Frontiers in Physiology, 13, 796097. Retrieved from https://pubmed.ncbi.nlm.nih.gov/35250609/
Niedermeier, M., Fröhlich, K., Frühauf, A., & Kopp, M. (2021). Psychological effects of calisthenic exercises on neuroinflammatory and rheumatic diseases. Frontiers in Psychology, 12, 678075. Retrieved from https://pubmed.ncbi.nlm.nih.gov/34177728/
Owen, P. J., Miller, C. T., Mundell, N. L., Verswijveren, S. J., Tagliaferri, S. D., Brisby, H., … & Belavy, D. L. (2020). Exercise therapy for chronic low back pain. Cochrane Database of Systematic Reviews, (9). Retrieved from https://pubmed.ncbi.nlm.nih.gov/32997745/
Motor vehicle accidents can leave lasting effects on the muscles, ranging from soreness and stiffness to more severe injuries like tears and chronic weakness. In many cases, the force of impact disrupts muscle coordination, nerve communication, and normal movement patterns. This is why rehabilitation after an accident must go beyond pain relief—it should focus on retraining muscles so they can function properly again.
Chiropractic care, when paired with integrative therapies such as physical therapy, massage, and acupuncture, offers a multi-layered approach to muscle recovery. By addressing spinal alignment, nervous system function, tissue quality, and muscle strength, this type of care supports the body’s natural healing processes while reducing the risk of long-term complications (Denver Colorado Chiropractic, n.d.).
Understanding Muscle Injuries After an Accident
After a collision, muscles may sustain damage from direct trauma or from secondary effects like joint misalignment and nerve irritation. Common issues include:
Muscle strains and tears from overstretching during impact.
Protective muscle spasms that limit movement.
Scar tissue that reduces flexibility.
Compensation patterns where uninjured muscles overwork to protect damaged areas.
If these problems aren’t addressed, they can contribute to chronic pain, reduced mobility, and posture problems. Chiropractic care helps by correcting structural issues that interfere with normal muscle function, while integrative therapies work to restore tissue health and strength (Pain Care LR, n.d.).
Chiropractic Care’s Role in Muscle Retraining
Chiropractic adjustments target misalignments that can disrupt nerve signals to muscles. Without clear nerve communication, muscles may remain tense, weak, or poorly coordinated. Adjustments restore alignment, reduce nerve irritation, and create an environment where muscles can respond better to rehabilitation exercises (Dallas Accident and Injury Rehab, n.d.).
A key part of post-accident chiropractic care is neuromuscular reeducation—teaching muscles how to activate properly again. This may involve guided movements, postural corrections, and targeted stretches or strengthening exercises. The aim is to break faulty movement patterns and replace them with balanced, efficient ones (My Evolve Chiropractor, n.d.).
Physical Therapy and Active Rehabilitation
Physical therapy is often combined with chiropractic care to provide the active component of muscle retraining. After an accident, therapeutic exercises help restore flexibility, strength, and coordination. These can include:
Gentle range-of-motion activities.
Isometric and resistance-based strengthening.
Balance and stability training.
Functional movement drills to prepare for daily activities.
Massage therapy works on the muscles and connective tissues to reduce tension, break up scar tissue, and improve circulation. Techniques such as myofascial release and trigger point therapy target problem areas, making muscles more responsive to adjustments and exercise (Utah Accident Clinic, n.d.; Synergy Healthcare Partners, 2024).
Massage also stimulates nerve endings, helping the brain reestablish correct muscle activation patterns. This makes it an important step in neuromuscular reeducation and overall recovery.
Acupuncture and Integrative Medicine
Acupuncture is another therapy often used in accident recovery. It can help reduce inflammation, relax tight muscles, and improve blood flow to injured tissues. Many rehabilitation programs now include acupuncture alongside chiropractic, massage, and physical therapy to create a holistic healing plan (Got Core, n.d.).
An integrative medicine approach looks at the whole person—not just the injury site—considering posture, daily habits, nutrition, and stress levels as part of the recovery process.
Advanced Diagnostics in Muscle Injury Recovery
Accurate assessment is critical before starting any rehabilitation plan. Advanced imaging, such as MRI or ultrasound, helps identify hidden injuries like deep muscle tears, scar tissue, or nerve compression that may not be obvious in a physical exam. These findings guide targeted treatment and ensure that muscle retraining addresses the root problem (Roach Chiropractic, n.d.).
Preventing Long-Term Complications
Effective muscle rehabilitation after an accident should focus on long-term stability, not just short-term relief. Ongoing care may include maintenance chiropractic adjustments, home exercises, and periodic massage or acupuncture to maintain flexibility and muscle balance. This reduces the risk of chronic pain, compensatory injuries, and recurrent strains (Mass General Brigham, n.d.).
Conclusion
Chiropractic and integrative care offer a comprehensive solution for retraining muscles after a motor vehicle accident. By combining spinal alignment, muscle reeducation, soft tissue therapy, and whole-body wellness strategies, patients can restore function, prevent reinjury, and return to their normal activities with greater confidence and comfort.
Learn about effective chiropractic care techniques to help relieve fibromyalgia symptoms and promote better health.
Fibromyalgia and Chiropractic Care: A Holistic Approach to Pain Relief and Musculoskeletal Health
Fibromyalgia is like that uninvited guest who shows up to the party and refuses to leave, bringing along a suitcase full of aches, pains, and exhaustion. For the millions of people living with this chronic condition, daily life can feel like navigating a maze blindfolded. The good news? Chiropractic care, especially from experts like Dr. Alexander Jimenez, DC, APRN, FNP-BC at ChiroMed – Integrated Medicine in El Paso, TX, offers a beacon of hope. This comprehensive, SEO-optimized blog post—crafted for a high school reading level—dives deep into how fibromyalgia impacts the musculoskeletal system, disrupts daily routines, and creates overlapping risk profiles that amplify pain and discomfort. We’ll explore why chiropractic care is a game-changer, highlight Dr. Jimenez’s expertise in personal injury cases, and sprinkle in some light humor to keep things engaging. Let’s get started on this journey to better health!
Understanding Fibromyalgia: The Basics
Imagine waking up feeling like you’ve been wrestling a grizzly bear all night, only to realize you just slept on your perfectly normal mattress. That’s the reality for many with fibromyalgia, a chronic condition that affects about 4 million adults in the United States, according to the Centers for Disease Control and Prevention (CDC). It’s characterized by widespread musculoskeletal pain, debilitating fatigue, sleep disturbances, and a foggy brain that makes you forget where you parked your car—or why you even walked into a room.
Fibromyalgia is a bit like a mystery novel with no clear ending. Its exact cause isn’t fully understood, but researchers point to a mix of genetic, environmental, and neurological factors. One key player is central sensitization, where the brain and spinal cord amplify pain signals, making even a light touch feel like a sledgehammer (Clauw, 2014). Another factor is oxidative stress, where an imbalance of free radicals and antioxidants damages tissues and fuels inflammation (Cordero, 2010). It’s like your body’s internal wiring is short-circuiting, sending pain signals on overdrive.
Fibromyalgia doesn’t just affect one part of the body—it’s a whole-body experience that can make everything from brushing your teeth to walking the dog feel like a Herculean task. To understand how chiropractic care can help, we first need to explore how fibromyalgia wreaks havoc on the musculoskeletal system.
References Clauw, D. J. (2014). Fibromyalgia: A clinical review. JAMA, 311(15), 1547–1555. https://doi.org/10.1001/jama.2014.3266 Cordero, M. D. (2010). Oxidative stress in fibromyalgia: From pathology to treatment. Current Rheumatology Reviews, 6(3), 178–183. https://pubmed.ncbi.nlm.nih.gov/
Fibromyalgia’s Impact on the Musculoskeletal System
The musculoskeletal system—your bones, muscles, tendons, ligaments, and joints—is like the scaffolding that holds your body together, letting you move, dance, or even binge-watch your favorite show comfortably. Fibromyalgia, however, throws a wrench into this system, causing pain and dysfunction that can make you feel like you’re stuck in a body that’s betraying you. Let’s break down how fibromyalgia affects this critical system.
1. Widespread Pain and Tender Points
Fibromyalgia is like the world’s worst interior decorator, scattering pain across your body with no rhyme or reason. It often targets specific “tender points” like the neck, shoulders, back, hips, and knees, which become hypersensitive to touch. Research shows this is due to central sensitization, where the nervous system misfires, amplifying pain signals (Sluka & Clauw, 2016). It’s like your body’s pain dial is stuck on “maximum,” making even a friendly pat on the back feel like a karate chop.
2. Muscle Stiffness and Fatigue
Ever felt like you’re moving through molasses, with muscles that refuse to cooperate? That’s fibromyalgia’s muscle stiffness at work. It causes muscles to feel tight and achy, even if you haven’t been to the gym or lifted anything heavier than a coffee cup. This stiffness can limit your range of motion, turning simple tasks like reaching for a shelf or tying your shoes into a full-body workout.
3. Joint Pain and Reduced Mobility
While fibromyalgia isn’t an inflammatory condition like arthritis, it can still make your joints feel like they’ve been replaced with rusty hinges. This joint pain and stiffness reduce mobility, making it hard to stay active. The result? A vicious cycle where less movement leads to more stiffness, which leads to more pain. It’s like your body is saying, “Move it or lose it—but good luck moving!”
4. Postural Imbalances
Chronic pain often leads to compensatory movements. If your lower back hurts, you might slouch or shift your weight to one side, throwing off your posture. Over time, these imbalances strain muscles and joints, creating secondary pain and dysfunction. Picture your body as a Jenga tower—every misaligned move risks toppling the whole structure.
5. Overlapping Risk Profiles
Fibromyalgia doesn’t travel alone—it often brings along buddies like chronic fatigue syndrome, migraines, and irritable bowel syndrome, which amplify musculoskeletal issues. These overlapping conditions create a cascade of risks, including muscle weakness, joint instability, and increased injury susceptibility. Poor sleep, a common fibromyalgia symptom, impairs muscle recovery, while stress heightens pain perception, further taxing the musculoskeletal system (Choy, 2015). It’s like fibromyalgia is throwing a party, and all the guests are causing trouble.
Living with fibromyalgia is like trying to play a video game on expert mode with a glitchy controller. The pain, fatigue, and brain fog make everyday tasks feel like epic quests. Here’s how fibromyalgia can turn your daily routine upside down:
1. Morning Misery
Mornings are often the worst for fibromyalgia sufferers. Waking up with stiff, achy muscles feels like you’ve been sleeping on a bed of rocks. Simple tasks like getting out of bed, brushing your teeth, or pouring cereal can feel exhausting, setting a challenging tone for the day.
2. Work Woes
Whether you’re crunching numbers at a desk or hustling on your feet, fibromyalgia makes work a struggle. Prolonged sitting or standing worsens pain, while fibro fog clouds your focus, making it hard to remember deadlines or follow conversations. Imagine trying to give a presentation when your brain feels like it’s stuck in quicksand—that’s fibro fog.
3. Exercise Challenges
Exercise is vital for health, but fibromyalgia makes it a tightrope walk. Gentle movement can help, but overdo it, and you’re sidelined with a flare-up. It’s like your body is saying, “Sure, go for a jog, but don’t be surprised if I send you an invoice for the pain later.”
4. Social Struggles
Chronic pain can make socializing feel like running a marathon. Canceling plans or skipping family gatherings becomes common, leading to isolation and strained relationships. Even playing with kids or pets can be tough when every movement feels like a chore.
5. Emotional Impact
The constant battle with pain and fatigue can lead to anxiety, depression, and frustration. It’s hard to stay upbeat when your body feels like it’s working against you. This emotional toll can amplify pain, creating a feedback loop that’s tough to escape.
These disruptions show why fibromyalgia isn’t just a physical condition—it’s a whole-life challenge that demands a comprehensive approach to manage effectively.
Why Chiropractic Care Is a Game-Changer for Fibromyalgia
Enter chiropractic care, the superhero of non-invasive, holistic health solutions. At ChiroMed – Integrated Medicine in El Paso, TX, Dr. Alexander Jimenez and his team are using chiropractic techniques to help fibromyalgia patients find relief and reclaim their lives. But how does chiropractic care tackle this complex condition? Let’s explore the clinical rationale, with a dash of humor to keep things light.
1. Taming Central Sensitization
Fibromyalgia’s calling card is central sensitization, where the nervous system turns every sensation into a pain signal. Chiropractic adjustments, especially spinal manipulations, stimulate mechanoreceptors (sensors in joints and muscles), which can dial down pain signal transmission to the brain (El Paso Chiropractor Blog, 2016). It’s like turning down the volume on your body’s overzealous pain alarm system.
2. Restoring Spinal Alignment
Spinal misalignments, or subluxations, can worsen pain and muscle tension. Chiropractic adjustments correct these misalignments, improving nerve function and easing stress on the musculoskeletal system. Think of it as realigning the tracks so your body’s train runs smoothly again, without derailing into Painville.
3. Boosting Mobility and Reducing Stiffness
Gentle chiropractic techniques, like spinal mobilization and soft tissue therapy, loosen tight muscles and joints, improving range of motion. For fibromyalgia patients who feel like they’re stuck in a suit of rusty armor, this is a game-changer. Regular adjustments keep the musculoskeletal system limber, reducing the risk of compensatory injuries.
4. Easing Inflammation
While fibromyalgia isn’t primarily inflammatory, chronic pain can trigger low-grade inflammation. Chiropractic care may help by improving blood flow and supporting the body’s natural healing processes, potentially reducing oxidative stress (Cordero, 2010). It’s like giving your body a mini detox, minus the green juice cleanse.
5. Supporting Holistic Wellness
At ChiroMed, chiropractic care is part of a bigger picture that includes nutrition counseling, rehabilitation, and stress management. This holistic approach addresses the root causes of fibromyalgia, helping patients build resilience and reduce flare-ups. It’s like assembling a superhero team to fight fibromyalgia from every angle.
6. Tackling Overlapping Risk Profiles
Fibromyalgia’s buddies—chronic fatigue, poor sleep, and stress—can worsen musculoskeletal issues. Chiropractic care helps by improving sleep quality (through pain reduction) and supporting overall wellness, mitigating these risk profiles. It’s like solving the whole puzzle, not just one piece.
Dr. Alexander Jimenez: El Paso’s Go-To Expert for Fibromyalgia and Personal Injury
In the heart of El Paso, Dr. Alexander Jimenez stands out as a trusted ally for those battling fibromyalgia and navigating personal injury cases. With over 25 years of experience as a chiropractor and family nurse practitioner, Dr. Jimenez brings a unique blend of clinical expertise and compassion to ChiroMed – Integrated Medicine (ChiroMed, n.d.). His LinkedIn profile showcases his dedication to holistic healing, combining chiropractic care, functional medicine, and advanced diagnostics (Jimenez, n.d.).
Personal Injury Expertise in El Paso
El Paso sees its fair share of personal injury cases, from car accidents to slip-and-falls. These incidents can exacerbate fibromyalgia symptoms, as trauma to the musculoskeletal system amplifies pain and stiffness. Dr. Jimenez is a distinguished practitioner in this field, known for his ability to bridge medical care and legal documentation. Here’s how he makes a difference:
Advanced Imaging and Diagnostics: Dr. Jimenez uses state-of-the-art imaging, like MRI and X-rays, to pinpoint injuries with precision. This helps identify issues that may worsen fibromyalgia or complicate recovery, ensuring accurate diagnoses.
Dual-Scope Procedures: As both a chiropractor and a family nurse practitioner, Dr. Jimenez employs a dual-scope approach, blending chiropractic adjustments with medical evaluations. This comprehensive care addresses both acute injuries and chronic conditions like fibromyalgia.
Legal-Medical Liaison: Personal injury cases require detailed medical documentation for legal claims. Dr. Jimenez acts as a liaison, providing thorough reports that link injuries to clinical findings, helping victims secure fair compensation while meeting their medical needs.
Why It Matters
For fibromyalgia patients involved in personal injury cases, the stakes are high. A minor fender-bender can trigger a major flare-up, making daily life even harder. Dr. Jimenez’s expertise ensures these patients receive tailored care that addresses both their immediate injuries and chronic fibromyalgia symptoms, navigating the complex intersection of health and legal challenges.
Complementary Therapies: The Dream Team for Fibromyalgia Relief
Chiropractic care is like the quarterback of fibromyalgia treatment, but it shines brightest when paired with a strong supporting cast. At ChiroMed, Dr. Jimenez and his team offer a range of services that complement chiropractic care to tackle fibromyalgia head-on. Here’s the lineup:
1. Physical Therapy Modalities
Physical therapy strengthens muscles, improves flexibility, and reduces pain. Techniques like low-level laser therapy, ultrasound, and manual therapy have shown promise in fibromyalgia management (Assis et al., 2013). It’s like giving your muscles a motivational speech to get back in the game.
2. Nutrition Counseling
What you eat matters when you’re fighting fibromyalgia. Anti-inflammatory diets rich in antioxidants can help reduce oxidative stress, a key player in fibromyalgia’s pathology (Cordero, 2010). ChiroMed’s nutrition counseling helps patients fuel their bodies for healing, not just surviving.
3. Acupuncture
Acupuncture, offered at ChiroMed, can reduce pain and improve energy flow by targeting specific points. It helps calm the overstimulated nervous system, like hitting the reset button on your body’s stress meter.
4. Stress Management
Stress is like pouring gasoline on the fibromyalgia fire. Mindfulness, yoga, and relaxation exercises, part of ChiroMed’s holistic approach, can lower stress and improve pain tolerance. It’s like telling your nervous system, “Take a deep breath, we’ve got this.”
5. Rehabilitation
Rehabilitation programs at ChiroMed focus on restoring function through targeted exercises and therapies. These programs help fibromyalgia patients rebuild strength and mobility, reducing the risk of future injuries.
References Assis, M. R., et al. (2013). Efficacy of manual therapy on pain, impact of disease, and quality of life in the treatment of fibromyalgia: A systematic review. Pain Physician, 16(5), E493–E505. https://pubmed.ncbi.nlm.nih.gov/ Cordero, M. D. (2010). Oxidative stress in fibromyalgia: From pathology to treatment. Current Rheumatology Reviews, 6(3), 178–183. https://pubmed.ncbi.nlm.nih.gov/
The Science of Fibromyalgia: What’s Going On Under the Hood
To understand why chiropractic care works, let’s take a peek at the science behind fibromyalgia. Recent research has illuminated its complex mechanisms, and here’s the CliffsNotes version:
Central Sensitization: Fibromyalgia involves an overactive pain-processing system, where the brain and spinal cord amplify pain signals (Sluka & Clauw, 2016). Chiropractic adjustments may help modulate these pathways.
Oxidative Stress: An imbalance of free radicals and antioxidants damages tissues and worsens pain. Therapies that improve blood flow, like chiropractic care, can counteract this (Cordero, 2010).
Not Autoimmune (Yet): While some wonder if fibromyalgia is an autoimmune disorder, current evidence suggests it’s more about neurological and biochemical dysfunction than autoimmunity (Giacomelli et al., 2013).
Diagnosis Challenges: Fibromyalgia is diagnosed based on symptoms like widespread pain and fatigue, often using the American College of Rheumatology criteria. Advanced diagnostics, like those used by Dr. Jimenez, help rule out other conditions (Häuser et al., 2017).
These insights highlight why a multi-faceted approach, like ChiroMed’s, is so effective—it tackles fibromyalgia from multiple angles, addressing both symptoms and root causes.
References Sluka, K. A., & Clauw, D. J. (2016). Neurobiology of fibromyalgia and chronic widespread pain. Neuroscience, 338, 114–129. https://doi.org/10.1016/j.neuroscience.2016.06.006 Cordero, M. D. (2010). Oxidative stress in fibromyalgia: From pathology to treatment. Current Rheumatology Reviews, 6(3), 178–183. https://pubmed.ncbi.nlm.nih.gov/ Giacomelli, C., et al. (2013). Is fibromyalgia an autoimmune disorder? Autoimmunity Reviews, 12(8), 790–795. https://pubmed.ncbi.nlm.nih.gov/ Häuser, W., et al. (2017). The diagnosis of fibromyalgia syndrome. Deutsches Ärzteblatt International, 114(22–23), 393–399. https://pubmed.ncbi.nlm.nih.gov/
Practical Tips for Managing Fibromyalgia
Living with fibromyalgia is like trying to herd cats while riding a unicycle—it’s tricky, but not impossible. Here are some practical tips, inspired by ChiroMed’s holistic approach, to help you manage symptoms and improve your quality of life:
Stay Active (Gently): Low-impact exercises like walking, swimming, or yoga can boost mobility without triggering flare-ups. Start small and listen to your body.
Prioritize Sleep: Create a relaxing bedtime routine and stick to consistent sleep schedules. A good night’s sleep can reduce pain and fatigue.
Eat Smart: Focus on anti-inflammatory foods like fruits, vegetables, and omega-3-rich fish. Skip the processed foods and sugar, which can fuel inflammation.
Manage Stress: Try mindfulness, meditation, or deep breathing to keep stress in check. It’s like giving your nervous system a warm hug.
Seek Professional Care: Regular chiropractic visits at ChiroMed can keep your musculoskeletal system in check and reduce pain.
Build a Support System: Connect with others who understand fibromyalgia through support groups or online communities. You’re not alone!
Conclusion: A Serious Note on Fibromyalgia and Chiropractic Care
Fibromyalgia is a complex condition that challenges every aspect of life, from physical health to emotional well-being. Its impact on the musculoskeletal system—causing widespread pain, stiffness, and reduced mobility—creates overlapping risk profiles that make daily tasks daunting. However, chiropractic care, led by experts like Dr. Alexander Jimenez at ChiroMed – Integrated Medicine in El Paso, TX, offers a powerful solution. By addressing central sensitization, improving spinal alignment, and supporting holistic wellness, chiropractic care can alleviate pain and enhance quality of life for fibromyalgia patients.
For those in El Paso dealing with personal injury cases, Dr. Jimenez’s expertise in advanced imaging, dual-scope procedures, and legal-medical liaison services ensures comprehensive care that bridges health and justice. His integrative approach, combining chiropractic care with physical therapy, nutrition, and stress management, tackles fibromyalgia from all angles, offering hope for lasting relief.
Disclaimer: This blog post is for informational purposes only and is not intended to replace professional medical advice. Fibromyalgia is a serious condition requiring individualized care. Always consult a qualified healthcare provider, such as Dr. Alexander Jimenez, DC, APRN, FNP-BC, for personalized diagnosis and treatment plans. For more information about ChiroMed’s services, visit https://chiromed.com/ or call (915) 412-6680.
Full Reference List
Assis, M. R., et al. (2013). Efficacy of manual therapy on pain, impact of disease, and quality of life in the treatment of fibromyalgia: A systematic review. Pain Physician, 16(5), E493–E505. https://pubmed.ncbi.nlm.nih.gov/
ChiroMed. (n.d.). ChiroMed – Integrated Medicine, holistic healthcare in El Paso, TX. https://chiromed.com/
Cordero, M. D. (2010). Oxidative stress in fibromyalgia: From pathology to treatment. Current Rheumatology Reviews, 6(3), 178–183. https://pubmed.ncbi.nlm.nih.gov/
Giacomelli, C., et al. (2013). Is fibromyalgia an autoimmune disorder? Autoimmunity Reviews, 12(8), 790–795. https://pubmed.ncbi.nlm.nih.gov/
Häuser, W., et al. (2017). The diagnosis of fibromyalgia syndrome. Deutsches Ärzteblatt International, 114(22–23), 393–399. https://pubmed.ncbi.nlm.nih.gov/